Concern is often expressed as to the adequacy of vegetarian diets, particularly in relation to their ability to supply sufficient micronutrients. In this section the vitamin and mineral status of vegetarians will be briefly discussed, and we will take a look at the role of food additives, alcohol, and the consumption of alkaloid-rich beverages in nutrition.
Vitamins and Minerals in vegan diets
To this day, vegetarian diets are considered to be deficient in many ways. Invariably the negative issues raised are protein, vitamin A, vitamin B-6, vitamin B12, vitamin D, iron, zinc and calcium adequacy. Omnivorous diets, on the other hand, are regarded as exemplars of dietary adequacy, and the impression is created that without adequate consumption of at least dairy products, serious dietary shortages will arise. Modern research has, however, shown that most of these assumptions are incorrect, and the reverse may indeed be true. Most vegetarian diets fare well when they are compared in their adequacy with dietary patterns of non-vegetarians. Vegans, vegetarians and whole-food omnivores whose diets were compared with those of the general public, were found to be exemplars of balance, variety and moderation. Also they were more in line with current dietary recommendations for nutrient intakes than were omnivorous diets.1
The explosion of knowledge in the last decades has made mankind acutely aware of all the possible dietary shortages which may arise. The fear of deficiency diseases, together with the inroads made by manufacturers of dietary supplements has led to a large-scale increase in intake of dietary supplements. However, dietary deficiencies in vitamins and minerals will only arise if impoverished diets are followed or if stress and disease place additional demands on the system. It is possible to exist without vitamin and mineral supplementation (as has mankind for much of its existence), a fact that has also been recognized by health organizations.2
Most people in the Western world consume huge quantities of vitamins and minerals in the form of supplements, and it has been found that a very real danger of potential toxicity exists in some of these cases. Supplement use is greater in females than in males, and the data suggests potentially harmful levels of vitamins A, C and E were being consumed, with some people consuming up to 275 000 IU/day of vitamin A. This is 55 times the Recommended Dietary Allowance (RDA). It was also found that more than 50% of people who consumed mineral supplements exceeded the RDA of iron, zinc and calcium whilst many consumed more than five times the RDA for calcium and iron.3 Excessive mineral intake can also impact negatively on health.4 Nevertheless, moderate dietary supplementation has its place, particularly in the case of children, and in cases where research has indicated that additional vitamins might be required. A detailed analysis of the vitamin and mineral composition of specific foods will be presented in chapter 7, and only those micronutrients which are of special interest to vegetarians will be discussed here.
Vitamin A
The World Health Organisation (WHO) estimates that 40 million children in the world suffer from vitamin A deficiency, but the incidence varies greatly from region to region. Approximately 350 000 infants and young children become blind annually because of vitamin A deficiency, and 70% of these die within one year.5 In a number of supplementation studies carried out in affected areas, it was found that there was on average a 33% reduction in mortality after supplementation, even though some studies reported no effect.6 Vitamin A (Retinol) is one of the fat-soluble vitamins, and it has a variety of functions. Vitamin A is one of the recognized anti-cancer vitamins in view of its antioxidant properties, but it also affords protection against infectious diseases, is essential for the formation of eye pigment, plays a critical role in growth and bone remodelling, maintenance of a healthy skin and epithelia, such as those of the respiratory tract and gastrointestinal tract, and it also plays a role in spermatogenesis and embryonic development.7 The need for vitamin A is increased in adolescents, and pregnant women require some 25% more vitamin A than non-pregnant women.8,9
Preformed vitamin A is found only in animal sources as it is usually associated with lipids, but provitamin A (β-carotene), the original source of retinol, is found in plant pigments. Vitamin A concentrations in the literature are normally given in International Units (IU). One IU is the equivalent to the biological activity of 0.3 mg of retinol or 0.6 mg of β-carotene. In 1974 the food and Nutrition Board of the US National Research council decided to replace the IU with the Retinol Equivalent (RE), as this measure accounts for the absorption and conversion of carotene to retinol. The equivalents of this unit are:
1 RE = 1mg retinol (3.33 IU)
1 RE = 6mg beta carotene (10 IU)
1 RE = 12mg other carotenoids (10 IU)
It thus takes six times more -carotene than retinol to meet the bodies needs, but on a vegan diet with plenty of fruits and vegetables, there is virtually no possibility of suffering from a vitamin A deficiency. In fact, oversupply can be a real danger especially in cases where large doses are taken as supplements. In its final state (as retinol) vitamin is toxic, and taking more than the recommended amount will lead to hypervitaminosis A the symptoms of which are fatigue, nervousness, headaches, dizziness and decalcification of bones. Vitamin A is poorly supplied in most meat dishes with the exception of liver, some fish and dairy products. RDA of vitamin A for adults is 1 000 RE/day for men and 800 RE/day for women. Vitamin A is moderately unstable and it is destroyed by heat, light, exposure to oxygen and acids. Diets rich in cooked animal products are thus not the best source of vitamin A. Provitamin A is, however, well retained in cooked vegetables, and a varied diet which includes pigmented fruits (particularly red and yellow) and green and yellow vegetables will supply ample vitamin A. Deficiency diseases in poor countries can be ascribed to a lack of fruits and vegetables in the diet and the fact that the diets of the underprivileged consist largely of grains which on the whole are poor suppliers of vitamin A.
Vitamin B-6
Vitamin B-6 is the name for three compounds that are precursors for this vitamin (pyridoxine,
pyridoxal and pyridoamine). Pyridoxal phosphate functions as a co-enzyme and it plays an important role in many enzyme reactions. Vegan vegetarians may have a lower vitamin B-6 status than the general public because certain factors in plants may influence the bio-availability of this vitamin. The presence of certain fibre types in the diet may inhibit the uptake of vitamin B-6. Some investigations show that the addition of cooked wheat-bran can reduce the bio-availability of the vitamin by 17% or less.10 However, the presence of cellulose, lignin or pectin has little effect on the absorption of vitamin B-6. Another factor which seems to affect the bio-availability of the vitamin is the presence of pyridoxine glucoside which is found in some plant foods, particularly the crucifers (cabbage family), and which can substantially reduce the availability of vitamin B-6. Finally the processing of foods also impacts on the availability of vitamin B-6. Thermal processing reduces the availability from animal products, and processing foods with a high vitamin C content has the same effect.11 Good plant sources of vitamin B-6 include whole grains, legumes and green leafy vegetables. In view of the factors that influence the availability of the vitamin, it is advisable to follow a varied whole-food diet. Whole foods are rich in fibre, and such a regime would eliminate the need for added bran. If care is taken to prepare vegetables in waterless cookware or by steaming, then the loss of vitamins through leaching will also be reduced to a minimum. Variety is, however, the most important watchword, and if practised, then there is no need for the elimination of any foods which may on occasion interfere with the uptake of vitamin B-6.
Vitamin B-12
Vitamin B-12 (cobalamin) is a complex molecule that contains the minerals cobalt and phosphorous. The vitamin is an important co-enzyme required for the metabolism of carbohydrates, proteins and fats. It functions together with folacin and plays an important role in DNA synthesis and the maturation of red blood cells. Severe vitamin B-12 deficiency can result in pernicious anaemia and can lead to irreversible neurological deterioration.
Plants do not produce vitamin B-12 and neither do animals. The vitamin is produced by bacteria, and animals thus obtain their supply from their intestinal bacteria, or from eating the flesh of animals. The bacteria that produce vitamin B-12 are very sensitive to acid and so they are confined to intestinal regions that have a low acidity. For ruminants there is thus no problem, as the rumen contains an alkaline medium and ample bacteria which can produce the vitamin. In non-ruminant plant eaters such as rodents and rabbits, the bacteria that produce vitamin B-12 are mainly confined to the posterior portions of the intestinal tract where absorption of the vitamin is minimal. They solve this problem through the phenomenon known as coprophagy (eating one’s own excreta), and thus satisfy their vitamin B-12 demands. Carnivores, in turn, obtain their supply of vitamin B-12 from the stored vitamin in the flesh of animals, but they also prefer to eat the rumen content of their prey, which is rich in nutrients, including vitamin B-12.
The human digestive tract also contains the bacteria which produce vitamin B-12, but these bacteria are again largely confined to the colon, where absorption is minimal or non existent because of the absence of the intrinsic factor required for its absorption.. The bacteria are there, and b -12 is produced in the colon as was proved by correcting vitamin B-12 shortages with extracts of human stools.12 Short of coprophagy, there is thus no other way of obtaining vitamin B-12 but through the diet. As plants do not produce vitamin B-12 (although there is evidence that some plants may produce small amounts), the vegan vegetarian can only obtain this vitamin from food that is contaminated with bacteria, or from the small amounts which are available from the intestinal bacteria. Vegan vegetarians have a high consumption of fibre, and as a consequence, they have higher concentrations of bacteria in the lower portions of the small
intestine where B-12 can still be absorbed because of a high enough concentration of the necessary intrinsic factor.13 The bacterial flora in the mouth can also contribute to the vitamin B-12 requirements of vegans.13 The more alkaline the diet, the higher the intestinal bacterial concentration will be, and great care should thus be taken to ensure proper food combinations and to consume correct proportions of alkaline to acid forming foods.
The requirements for vitamin B-12 are extremely low, and nobody needs more than 1 mg/day. It has even been found that doses as low as 0.1 mg/day could reverse symptoms of deficiency.14 Moreover, vitamin B-12 is reabsorbed very efficiently from bile and thus has the longest reserve capacity of all vitamins, and this explains why it takes up to 20 years to run out of vitamin B-12 after one stops consuming it. In cases of disturbed absorptive capacity, mostly because of intestinal infections or a reduction in the production of the intrinsic factor required for the absorption of vitamin B-12 it will however take only 3 years to run out of vitamin B-12.14 The production of the intrinsic factor is normally impaired when portions of the stomach have been operatively removed, or if there is an infection of the stomach mucosa (gastritis). This probably explains why cases of vitamin B-12 deficiency are rarely reported in the literature.6 Vegan vegetarians need thus not panic over the issue, but they should be aware of the possible shortages which may arise, particularly in small children, and should supply the lack in the form of a supplement or foods fortified with cobalamin. Fortified soy milk or vitamin B-12 fortified nutritional yeast are possible sources for this purpose. It is important to ensure sufficient dietary B-12 in the case of infants that are breast fed, as B-12 reserves will decline over time in mothers that breast feed if reserves are not maintained.13 For peace of mind in this regard, it would be prudent to have a serum analysis done to determine the concentrations of B-12 in the blood, as this is the most accurate way of determining B-12 status.
When purchasing fortified foods or supplements, it is important to note that the product contains cobalamin, and not some analogue of the vitamin. Most of the claims of B-12 content on products are incorrect, as the analysing techniques used do often not distinguish between analogues and the active B-12 which is cobalamin. Fermented soy foods, such as tempeh, also do not contain vitamin B-12, and neither does Spirulina, which is often sold in health shops as a source of vitamin B-12.14 Spirulina may even make matters worse because it contains analogues which may interfere with normal absorption of cobalamin.
Vitamin D
Vitamin D is really a pro-hormone, and its active form is the hormone 1,25-dihydroxycholecalciferol [1,25 (OH)2D3]. The two compounds with vitamin D activity are ergocalciferol (vitamin D2) and cholecalciferol (vitamin D3). Vitamin D2 is found in ergot, a fungus growth on cereals, and vitamin D3 is formed when the skin is exposed to sunlight. The vitamins are also found in yeast and the oil of fishes. Vitamin D is fat-soluble, and requires the presence of bile salts in order to be absorbed from the intestines. Vitamin D is essential for the absorption and transport of phosphorous and calcium, and it promotes normal bone mineralisation. Deficiencies result in malformation of the bone structure in growing children, a condition known as rickets.
Since vitamin D does not occur in plants per se, it is possible to develop shortages of this vitamin if exposure to the sun is minimal. Vegans living in sunshine-poor areas should thus provide some form of supplementation to children and infants in particular. Nutritional rickets may occur in infants if the nursing mothers are themselves deficient in vitamin D.8 It is therefore, advisable for nursing mothers, in sunshine-poor areas, to also take a vitamin D supplement. Margarines are normally fortified with vitamin D, but if oils and margarines are
avoided, then supplementation through tablets seems desirable in sunshine poor areas.
Iron
Iron deficiency is the most widespread nutrition problem in the world today. According to the WHO the incidence of iron deficiency in developing countries is 26% for men, 42% for women, 46% for school-age children and 51% for children 0 to 4 years of age.6 Iron is essential for the formation of haemoglobin and shortages will lead to anaemia. Iron, together with zinc and copper is also essential for maintaining immunocompetence. Deficiencies in either of these minerals will lead to increased susceptibility to infectious illnesses.15 An early symptom of iron deficiency is chronic tiredness, whereas dizziness, breathlessness, interference with body temperature regulation and constipation are further warning signs. In infants, iron-deficiency anaemia has been shown to delay psychomotor development and impair the cognitive performance, and deficiency in mothers during pregnancy increases maternal mortality, prenatal and perinatal infant loss and premerturity.6
Iron can enter into the body in two forms, nonhaeme iron and haeme iron. All the iron in plant foods is in the form of nonhaeme iron, whereas in animal tissues three fifths of the iron is in the form of nonhaeme iron and two fifths is in the form of haeme iron. Haeme iron is more readily absorbed than nonhaeme iron, and this has prompted the concern that vegetarians may suffer from iron deficiency. The RDA for iron is 10 mg/day for men and 18 mg/day for women in their childbearing years. In a recent survey of the relevant literature it was found that adult menstruating women need to absorb 2,84 mg/day of iron and, as only a fraction of the dietary iron is absorbed, this would require a dietary intake of 18,9 mg/day. Teen-age girls would require a somewhat higher intake of 21,4 mg/day. However, many factors, such as the type of contraceptive used and the type of diet consumed, impacted on iron requirements.16
Most vegetarians living in Western countries have less iron deficiencies than might be expected from the type of iron which they consume. One of the reasons for this phenomenon is that nonhaeme iron absorption is enhanced by other factors in the vegetarian diet. Vitamin C intake in vegetarians is normally high, and this enhances the uptake of iron, and can counteract the effect of absorption inhibitors such as phytate which acts as a chelator of iron. The mineral content of plant foods is often high, and this can also offset the effects of inhibitors. Black tea also contains high concentrations of inhibitors, which impact negatively on iron absorption and avoidance of this beverage is thus advisable. A further factor which can lead to inadequate iron absorption is a high calcium level in the diet.17 Finally it can be said that a vegetarian whole-food diet can supply all the iron requirements, provided a varied diet is followed, which includes a regular consumption of iron-rich foods as outlined in chapter 7.
Calcium (See also calcium in dairy products in chapter 4)
Calcium is the most abundant mineral in the human body. It is essential for a host of physiological functions and for the normal growth and development of the skeletal system. One of the most misrepresented issues in human nutrition is the issue of calcium, and some of these issues have already been discussed. In chapter 1 the negative impact of high protein, particularly animal-protein diets, on calcium absorption and storage was discussed, and in chapter 4 the availability of calcium from dairy products was also investigated. It was shown that most diets in affluent societies are directly responsible for calcium loss from bone, and that distinct correlations exist between the consumption of dairy products and the incidence of
osteoporosis. High-protein diets cause calcium loss in the urine, and animal proteins pose a greater risk than plant proteins.18,19,20,21,22 The reason for this is that sulphate (a product of protein metabolism) excretion is linked to calcium excretion.
High sodium diets also cause calcium loss via the urine as do diets rich in chloride.23 Calcium homeostasis is best achieved by a balanced relationship between macro- and micro-nutrients. Dietary excesses of anions seem to inhibit absorption of calcium, and dietary excesses of cations seem to cause calcium loss. Affluent diets and diets rich in animal products are usually high in sodium and can thus account for substantial calcium loss in the urine. In contrast, whole-food programmes will provide a superb relationship between the macro and micro nutrients, and will curtail the loss of urinary calcium. Some investigators have found that phytic acid (found in grains and legumes), may impact negatively on calcium absorption, but this issue has not yet been satisfactorily resolved as other investigators did not find similar results.23 Grains, legumes, nuts, some seeds and dark green vegetables, are excellent sources of calcium, and if care is taken to regularly include these calcium-rich foods in the diet, then concern for calcium deficiencies is unwarranted.
Zinc
The significance of zinc in the diet has only recently been appreciated. Zinc forms an important component of many enzymes known as metaloenzymes, of which many participate in the digestion and assimilation of nutrients. Zinc is also essential to the proper function of the endocrine system because it forms a structural component of the hormone receptor system.24 Moreover, zinc plays a role in the synthesis of RNA and DNA, and is essential for the proper functioning of the immune system.15
Most dietary guidelines will recommend the consumption of animal products as a source of zinc, but it has been found that, as in the case of calcium, the high protein content of diets rich in animal products impacts negatively on zinc availability.23,25 Incomplete hydrolysis of casein, the protein in milk, also inhibits the uptake of zinc.23 As in the case of calcium, phytate, found in grains and legumes, may inhibit the absorption of zinc, but this may be partially offset by the protein composition of these foods. Finally, it seems as if the toasting of foods renders the protein-phytate mineral complexes less digestible and leads to lower mineral availability.26
A vegetarian whole-food diet will supply more zinc than an omnivorous diet. Legumes and seeds have a relatively high zinc content ranging from 2.7-3.2mg/100g, and grains are also rich in zinc. The bran and the germ of wheat are the main storage area of zinc in grains and contain an average of 9.8 and 14.3mg/100g respectively.27 It is better to obtain zinc from whole foods, however, than from added bran and wheat-germ, as the high fibre content of such fortified meals will make the zinc less available. Vegetables and fruits are relatively low in zinc content, emphasizing the need for a varied diet which, beside fruits and vegetables, includes grains, seeds and legumes. The zinc content of selected plant foods is presented in table 6.1, and values for some animal products are given for comparison.
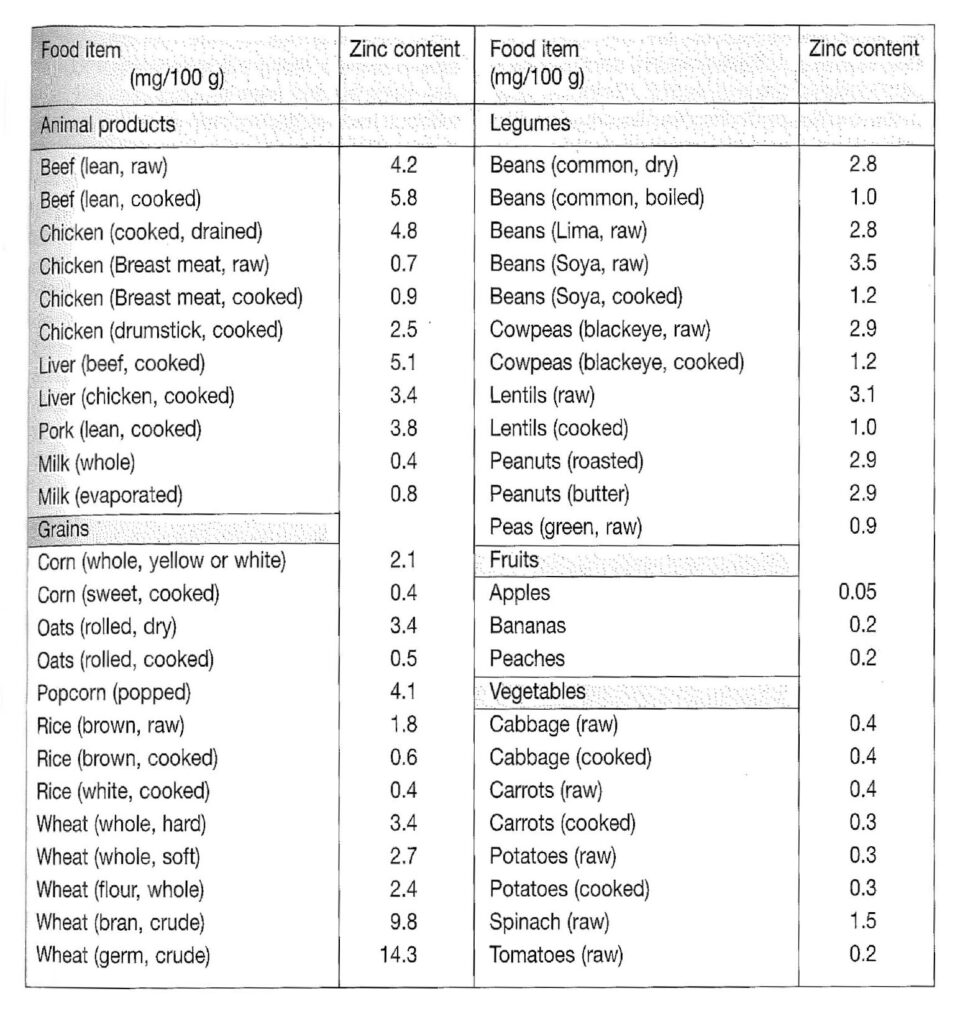
Table 6.1. The zinc content of selected foods. (Adapted from reference 27)
FOOD ADDITIVES
Food additives are substances which are added to food, but are not commonly regarded as food. These substances can be added at any stage of the manufacturing process and affect the keeping quality, texture, appearance, odour, acidity or alkalinity and the consistency of the food. Colorants, antioxidants, preservatives, emulsifiers and stabilizers as well as numerous miscellaneous additives such as sweeteners, solvents and improving agents fall into the category of food additives. In most countries their use is extensive, and they are controlled by comprehensive legislation. In the following discussion a brief overview of some commonly used additives is given, with discussions on their impact on health. It is not the intention to create the impression that all food additives are bad, or that the various legislative bodies permit the use of food additives without due consideration for the well-being of the consumer. However, a great deal of controversy surrounds the use of some of these substances, and the current scientific literature provides sufficient evidence for circumspection in their use.
The 1984 UK food act does not include vitamins and minerals, that are added to foods to fortify them, as additives, and neither are herbs and spices, hops, salt, yeast or yeast extracts, the products of food protein hydrolysis or autolysis, starter cultures, malt or malt extracts, air or water regarded as additives. Finally, substances that are in foods as a consequence of crop management or animal husbandry do also not fall under the regulations controlling food additives. This last category thus excludes substances such as pesticides, fumigants, sprout depressants, veterinary medicines and substances that are added to the feed of animals. In table
6.2 the European Community categories of food additive are listed and the table also contains information on the stage of functionality of the additives.
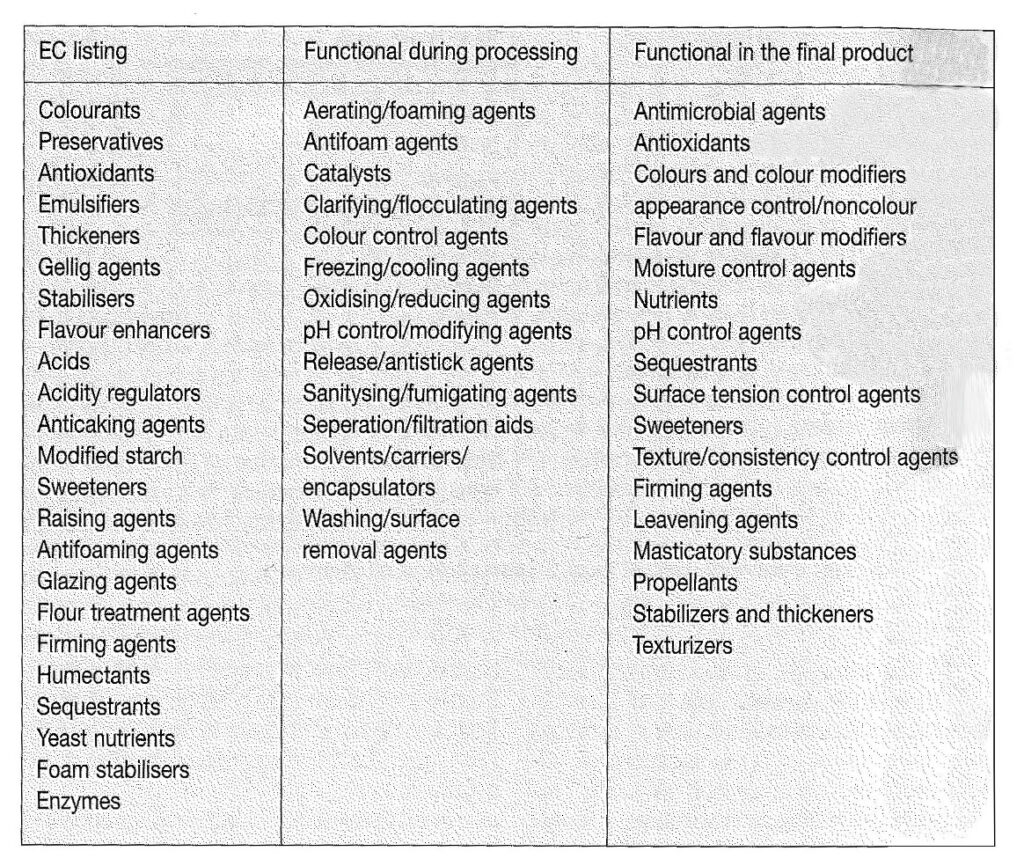
Table 6.2. List of food additives as defined by the EC and classification on the basis of their technical effects. (Adapted from references 28 and 29)
An extensive body of legislation guides the use of food additives on national and international levels. The international evaluation of the safety of Food Additives is undertaken by the Joint FAO/WHO Expert Committee on Food Additives (JECFA) which also develops specifications on the purity of these substances. In recent times there has been an increase in public awareness of the potential health effects of the thousands of food additives which are utilized by the food industry, but unfortunately sufficient information to make informed judgements on their safety is often lacking. The safety of additives is mostly assessed from long-term feeding trials, where additives are fed to experimental animals in doses which exceed those to which humans would generally be subjected, and the ADI (acceptable daily intake) is then determined. Although new compounds are subjected to this type of testing before they can be used as food additives, many substances that were in use prior to the new regulations, are used without knowledge of their potential toxicity. In the USA these compounds are listed, under a special clause, on the GRAS (Generally Regarded as Safe) list of food additives
The conventional methods of testing for toxicity are directed mainly at pathology, and effects on reproduction, embriotoxicity, tetragenicity and mutagenicity are normally assessed. There are, however, other criteria, which are equally as significant in determining the safety of food additives, which are not as readily resolved by conventional trials, and these include functional defects such as behavioural abnormalities and effects on the intelligence. Moreover, it is often difficult to pinpoint the levels of exposure to food additives, particularly as new products appear and old ones are replaced at rates which make long-term assessment difficult.30 The quantities of food additives which may be added to foods are only prescribed for certain
categories of additives, and in the case of colorants, emulsifiers, stabilizers, solvents and most miscellaneous additives, there are mostly no prohibitions as to the amounts of these substances which may be used in foods, although their use may be restricted to certain categories of foods. Maximum daily ingestion of some food additives has been estimated to be up to 100mg/day of azo colours, 50mg/day of non-azo colours, 200mg/day of antioxidants and 1g/day of benzoate products.31 It is, therefore not surprising that adverse effects, ascribed to food additives, are being reported more and more in the literature. Interest in this topic was stirred when Finegold, the paediatric allergist, who alleged that many children suffering from hyperactivity and minimal brain dysfunction were actually sensitive to certain constituents in their diet, singled out synthetic food colours and flavourant as being among the chief offenders.32 Finegold came under much criticism, but a large body of current research shows that his assertions cannot be summarily rejected.33 Much of the criticism revolves around the relatively low doses of additives to which humans are exposed, compared to clinical trials which take place in the laboratories. It must, however, be remembered that in clinical trials the animals are subjected to one agent at a time, whereas humans are subjected to numerous additives simultaneously. Moreover, laboratory rats are fed high-fibre diets, whereas modern Western diets are very low in fibre, and it has been established that low-fibre diets greatly magnify the toxic effects of colorants and other additives. Beside Finegold’s assertions, a surprising number of the symptoms associated with food allergies have been reported, and some of these are summarized in table 6.3.
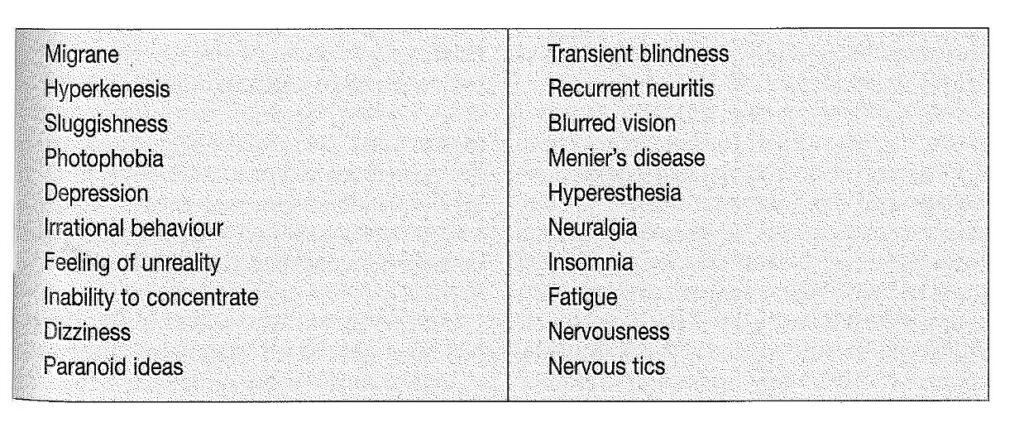
Table 6.3. Neurobehavioural reactions attributed to food allergy. (From reference 33)
Artificial and Natural Colorants
Colorants are used to make the food more acceptable to the consumer, but since many adverse reactions to artificial colorants have been reported, many of these have been banned in some countries and natural colorants are being used more frequently. In the UK some foods are not permitted to contain added colorants, namely raw meat, game, poultry, fish, fruit or vegetables, tea, coffee, condensed or dried milk, cream and certain types of bread. Bread, cheese and butter may contain a restricted number of dyes, and raw meat may be coloured with the basic dye methyl violet. Allergic reactions or intolerant responses have been reported for most of azo dyes used as food colorants, and in some countries (Norway) they have been banned. In other countries, including Sweden, Finland, Austria, Greece and Japan, their use has been severely restricted. Nevertheless, azo dyes are still used extensively throughout the world in spite of the reported health hazards.
Some of the more common azo colours include amaranth (red), azorbin (red), brilliant black, sunset yellow (yellow), carmousine and tartrazine (yellow), most of which are potential allergens as demonstrated in their potential to induce histamine release by leukocytes of normal and urticaria patients.31 A similar, though reduced potential, was also demonstrated for non-azo colours such as quinoline yellow, green S and indigo carmine. Colorants have been shown to induce asthma, rashes, hay fever, blurred vision and tummy upsets. Moreover their role in inducing hyperactivity and other behavioural disorders in children has been clearly established. In one study, a group of children on an additive-free diet, were given a
cookie containing a blend of eight food colours. Within three hours after the ingestion of the cookie some of the children showed impaired perceptual-motor performance and increased hyperactive behaviour with the greatest effect being on the youngest individuals.33,34 Impaired learning ability is another negative response to colorants, and some children develop a short attention span, whine and tend to throw tantrums.33
Azo compounds have also been reported to effect aggregation of platelets, and to have an inhibitory effect on both prostaglandin synthetase and thromboxane activity, though these claims have been challenged. Tartrazine in particular has been implicated in cases of acute urticaria angio-oedema, eczema, asthma, nausea and migraine attacks by impacting on the immune system.35,36 Some of the caramels, particularly ammonia caramel, have been shown to have lymphocyte depressing effects, and the orange/red colorant canthaxanthin, which is used to obtain artificial browning, has been found to produce crystalline deposits on the retina. Another red colorant, erythrosine, has been shown to affect thyroid function and may have oncogenic and carcinogenic effects. Concern about these issues has prompted a reduction of the ADI and NEL (no effect level) for most of these compounds.37 In the USA the colorant amaranth and ponceau 4R (red) are also banned.
Natural food colours are becoming increasingly popular, and the main classes are the carotenoids, beetroot extract, anthocyanins, riboflavins, cochineal, chlorophylls and naturally coloured foods such as paprika, turmeric, saffron, and sandalwood together with extracts of these materials. Though sensitivity to natural colorants is considerably lower than artificial colorants, in some cases they may also elicit a negative response. Overall it can thus be said that avoidance of food colorants can only be of advantage to the consumer.
Antioxidants
Antioxidants are added to oils and fats to prevent rancidity and normally this is best achieved when mixtures of antioxidants are used for this purpose. Natural antioxidants include some vitamins (particularly vitamin E and ubiquinols) and some phenolic compounds occurring in foods, especially spices. Most regulatory bodies permit the use of various gallates such as butylated hydroxyanisole (BHA) and butylated hydroxytoluene (BHT) in dairy products and fats. Some directives also regard calcium disodium EDTA as an antioxidant for use in salad dressings and mayonnaise. BHA and BHT are used mainly for the protection of unsaturated fats and oils as well as baked goods, cereals, nuts (particularly walnuts), milk powder and in dehydrated potato products such as potato chips and snacks.
The safety of these synthetic antioxidants has been questioned lately,38 and in the case of BHA sufficient evidence for carcinogenicity in experimental animals has been found to prompt changes (but not withdrawals) in the recommended usage of this compound.37,39 BHA has been shown to produce hyperplasia and/or tumours in the forestomach of rats, mice and hamsters.37 BHT, on the other hand, has been shown to have adverse effects on thyroid function, and haematological studies have also revealed that some, but not all, species show haemorrhaging effects and/or reduction in prothrombin index.38 Some evidence also exists for a carcinogenic effect of BHT, as demonstrated by two recent Danish and Japanese studies.37
The natural antioxidants, such as the tocopherols (vitamin E) and ubiquinols have a cyclic nucleus and a hydrocarbon tail, and the antioxidant properties are produced by the cyclic nucleus of these molecules. When these compounds form part of the membrane systems of cells, the orientation in cell membranes is, however, accomplished by the other components of the molecules. Synthetic antioxidants contain only the fragments which ensure the antioxidant properties of the compounds, and this may be the source of their destructive and perturbative action on cell membranes and can explain their toxicity.40 Natural antioxidants can be very
effective, and research has shown that they can compete with the synthetic varieties.41
Emulsifiers and stabilizers
Emulsifiers are used to disperse tiny globules of one liquid in another so that they will stay mixed. Their use has made it possible to market oil-containing foods, such as peanut butter and margarines, that will not separate and so are instantly usable. Emulsifiers are used extensively in the baking industry to help increase volume and to effect the fineness of the grain. Stabilizers and thickeners are used to bind together solids and liquids so that they will not separate. They are used in ice-cream, many cake and pudding mixes, cheese spreads, salad dressings, soups and many others too numerous to mention.
Most commercial stabilizers and thickeners are pure plant extracts, and the use of plant gums for this purpose, is quite extensive. Gums are extracted from seaweed, trees and seeds, while cellulose derivatives are obtained from wood pulp and cotton. The seaweed extracts include agar, algin, carrageenan and furcellaran. The tree gums include arabic, ghatti, karaya, larch and tragacanth. Then there are still extracts of seeds which include guar, and extracts from the carob bean, and finally the commonly used cellulose derivatives are methylcellulose, carboxymethyl-cellulose and hydroxypropyl-methylcellulose. The most commonly used natural emulsifier is lecithin which is obtained from soybeans and other vegetable oils, but synthetic mono-, di- and triglycerides are also extensively used. Synthetic stabilizers and emulsifiers are used extensively in the baking and dairy industry, and in the UK the permitted substances include stearyl tartrate, complete glycerol esters, partial glycerol esters, partial polyglycerol esters, propylene glycol esters, monosteatrin sodium sulphoacetate, Sorbitan esters of fatty acids and their polyoxyethylene derivatives, cellulose ethers, sodium carboxymethyl cellulose and acetic and tartaric acid esters of mono- and diglycerides. Some of these compounds are suspected to be carcinogens, and approval for the use of some of the polyoxyethylene compounds has been withdrawn in some countries.
Solvents
Solvents are used to dissolve raw materials and concentrates and they are also used to incorporate flavours, oils, colours, antioxidants and vitamins into foods. Many of the compounds used are considered to be health risks, and the use of some of these compounds has been banned in some countries. In the UK, solvents are categorized as carrier solvents, extraction solvents and processing solvents. The list of permitted solvents in the UK is presented in table 6.4. The list is extensive, and raises questions as to the desirability of consuming foods treated in this way, particularly since some are suspected of having carcinogenic properties.
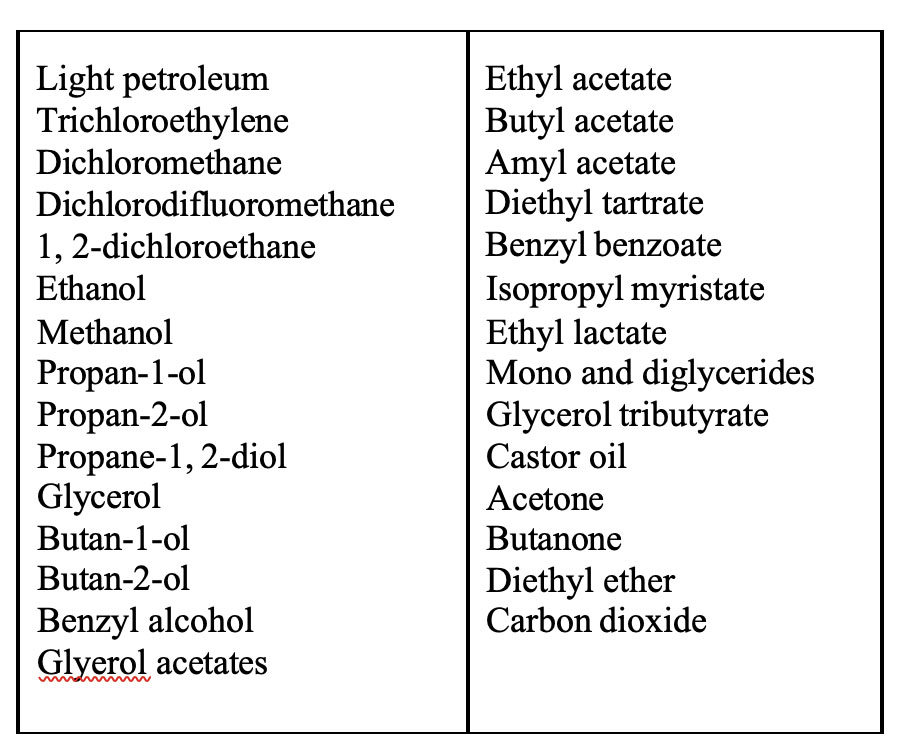
Table 6.4. The FACC recommended list of solvents.(From reference 28)
Preservatives
Preservatives are used to prevent the growth of mould, or as antimicrobials. Food preservation is a very old industry, and since ancient times food has been preserved by drying, smoking or by the addition of salt or sugar. Today, food preservation has become a huge industry, and beside the ancient methods, canning, bottling and refrigeration are extensively used to preserve foods. With the expansion of the chemical industry, however, the use of synthetic organic and inorganic preservatives has become fashionable in the food industry.
The most commonly used inorganic preservatives are sulphur dioxide, nitrates and nitrites. Sulphur dioxide is used in gaseous form, in solution as sulphurous acid, or as sulphites of sodium, potassium or calcium. It prevents the browning of foods and also inhibits the growth of moulds, and it is used extensively in the preservation of fruit juices and dried fruits. Sulphur dioxide is known to destroy vitamin B, but it helps to preserve vitamin C, however, its use is also associated with asthma.31 Sodium and potassium nitrate and nitrite are used mainly in the curing of meats and in some cheeses, but concern about their possible carcinogenic effect has prompted stricter control over these compounds in some countries. Their use is restricted in most European countries, and because they have the potential to form nitrosoamines and to interfere with the metabolism of infants and young children, they may not be used in infant foods in the UK.28
Nitrites have a powerful antimicrobial action, but they also influence the flavour and colour of the food. The pink colour of bacon and ham is due to their action on haemoglobin which is converted to nitrosohaemoglobin. Although the use of these compounds is restricted in infant foods, this does not prevent the consumption of treated foods by young children. Indeed, cured meats are advertised as the ideal food for growing children, an issue that should be of some concern to responsible adults. Sodium nitrite can also cause headaches, skin rashes and gut disturbances.4 Another prohibited inorganic preservative is boric acid which is not used because it is cumulative, however it is still used for the preservation of caviar.28
The most extensively used organic preservatives are benzoic acid, 4-hydroxybenzoates, salicylic acid, parachlorobenzoic acid, dehidroacetic acid, propionic acid, sorbic acid and sodium diacetate. Many of these products are used in the preservation of breads and flour confectionery. Benzoic acid and benzoates are used for the preservation of some jams, fruit juices, desserts, tinned fruits, salad creams, yoghurt, sauces and margarines. It is also an effective agent against the growth of yeasts and moulds. Benzoic acid is also a natural ingredient in some small berries. Benzoic acid has been implicated in urticaria and most of the symptoms associated with a sensitivity to tartrazine.35
Flavour enhancers
Monosodium glutamate (MSG) and the ribonucleotides disodium inosinate and disodium guanylate are commonly used as flavour enhancers in processed foods. The use of MSG is extensive, and annual world production of this compound exceeds 300 000 tons. MSG is a neurotoxin which effects the destruction of the arcuate nucleus (AR) of the hypothalamus when administered to mice.42,43 MSG is converted into the amino acid, glutamic acid, which is known to have neuroexcitory properties, and glutamate is also implicated in neurotransmission. Interest in MSG was stimulated after some people experienced symptoms such as tightening of the face and chest muscles and also a burning sensation in the upper body as well as headaches. This was called Chinese restaurant syndrome, because it was frequently experienced by patrons of Chinese restaurants and was traced to the liberal use of MSG by Chinese chefs.
Other symptoms associated with MSG are dizziness, diarrhoea, nausea and stomach cramps. Some children experience shudder attacks which may be mistaken for epilepsy, and long-term exposure in mice can lead to obesity.42,33 The most serious side effect of MSG is, however, its neurotoxic effect which also affects the endocrine function. MSG has been reported to depress growth hormone levels, and levels of prolactin and sex hormones are also affected.44,45,46 Such findings should make one extremely cautious of using MSG, and replacement products such as protein hydrolysates should also be avoided as they also contain large amounts of glutamate and thus have the potential to elicit similar effects.
Sweeteners
Non-carbohydrate sweeteners are divided into two classes, those with a sweetness similar to sucrose are called bulk sweeteners and those with a sweetness that greatly exceeds that of sucrose are known as intense sweeteners. Bulk sweeteners supply similar calories as sugar, but as they are not metabolized in the same way, they are used as substitutes for sugar in the preparation of diabetic foods and they are also used in foods that are stored at low temperatures such as ice-cream. Bulk sweeteners include hydrogenated glucose syrup, sorbitol, mannitol, xylitol, lactitol and isomalt. The intense sweeteners include the synthetic sweeteners (artificial sweeteners) saccharin, cyclamate, aspartame, acesulfam-K, thaumatin, stevioside, sucralose and alitame.
The most controversial sweeteners are the cyclamates and saccharin. Cyclamates are banned in many countries on the strength of laboratory experiments which indicated that they could be tetragenic and carcinogenic. The evidence for these phenomena is, however, controversial. The IARC monographs list saccharine as a chemical for which there is sufficient evidence for carcinogenicity,37,39 but it still remains on the list of approved food additives. Aspartame is another problem sweetener because its effect is similar to that of MSG.33
Although the above list of food additives is by no means complete, it should be clear that the issue is indeed worthy of some concern. Legislation governing the use of food additives is not equally explicit in all countries, but most responsible bodies realize their duty in keeping the public informed. In most countries there is legislation which enforces the proper labelling of food items sold to the general public, and most nutritional organizations support the right of the public to know what is in the food they buy. In the United States new labelling guidelines are being considered with this very purpose in mind. The positions of the American Institute of Nutrition, the American Society for Clinical Nutrition and the American Dietetic Association also clearly underscore the policy that sound nutritional information should be provided to the
American public. They, however, also acknowledge the fact that substantial improvement in nutrition education of the public is necessary for food labelling to serve its purpose effectively.47 The policy of comprehensive food labelling affords each individual the opportunity to make his own choice as to what foods he wishes to buy.
CAFFEINE AND ALCOHOL
No discussion on healthful living would be complete without reference to caffeine and alcohol. Both these compounds play a major role in human nutrition, and the sale of commodities containing either of these substances plays a major role in the economy of many nations. Tea, coffee and cocoa are important plant exports of many nations and in some cases they are the major, or only, earners of foreign exchange. The stimulating effects of tea, coffee and cocoa are due to their alkaloid content. Alkaloids are complex compounds containing carbon, hydrogen, nitrogen, and usually oxygen. The nitrogen often forms part of a heterocyclic ring system and as alkaloids are usually basic compounds, they normally form salts with acids.
The alkaloids found in tea, coffee and cocoa are caffeine, theobromine and theophylline. Caffeine is found in tea and coffee, whilst theobromine is found in cocoa. Tea also contains the alkaloid theophylline, but all of these compounds have a similar structure and are derived from purines (fig 6.1).
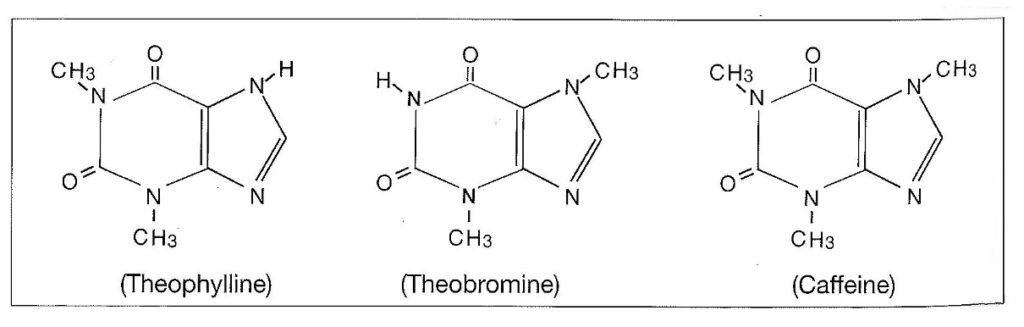
Figure 6.1 The structure of alkaloids found in tea, coffee and cocoa.
Tea (Camellia sinensis) has been used in China for thousands of years and it is cultivated extensively in Asian and African countries. Harvesting of tea takes place after flushing, which is the term used to describe the development of the new growth which occurs after pruning. For the “best” tea, only the two top leaves and the bud are used, but for coarse tea the bud and all four leaves of the flush are used. Plants protect their ephemeral (young) tissues from herbivory by concentrating secondary plant compounds, such as alkaloids, in these tissues, and it is therefore surprising that the ephemeral tissue is used to make tea. Green tea is produced by heating the harvested leaves to prevent fermentation, and black tea is produced by encouraging fermentation. After harvesting the leaves are spread out on nets to dry whilst hot air is blown over them. They are then crushed and polyphenols and enzymes are released and fermentation is initiated, which results in compounds that give tea its characteristic flavour. The “best” tea has high concentrations of polyphenols (called tannins, but are not the same as those used for tanning leather) which are also compounds that prevent herbivory in nature and affect the ability to digest, absorb and assimilate nutrients.
Coffee (Coffea spp) is grown largely in South America, the West Indies and Africa. The harvested berries are opened and allowed to ferment in water, and are subsequently dried in the sun to produce mild coffee. Hard coffee is prepared by first drying the beans and then removing the pulp. The beans are then roasted, which changes the sugars to caramel and gives the beans their dark colour. The cocoa plant (Theobroma cacao) is grown for its pods, which are also fermented, and the cocoa beans subsequently dried. The beans are roasted to drive off the acetic acid, which is formed during the fermentation process, they are then ground and can then be further separated into cocoa butter and cocoa powder. Cocoa powder contains approximately one per cent theobromine.
Caffeine
The consumption of caffeine begins at an early age for many people. Caffeine is a natural ingredient in tea, coffee and some soft drinks, and it is used as an additive in many baked goods, frozen dairy products, sweets, gelatins, puddings and soft drinks. The quantities of caffeine in some commonly used items are summarized in table 6.5.
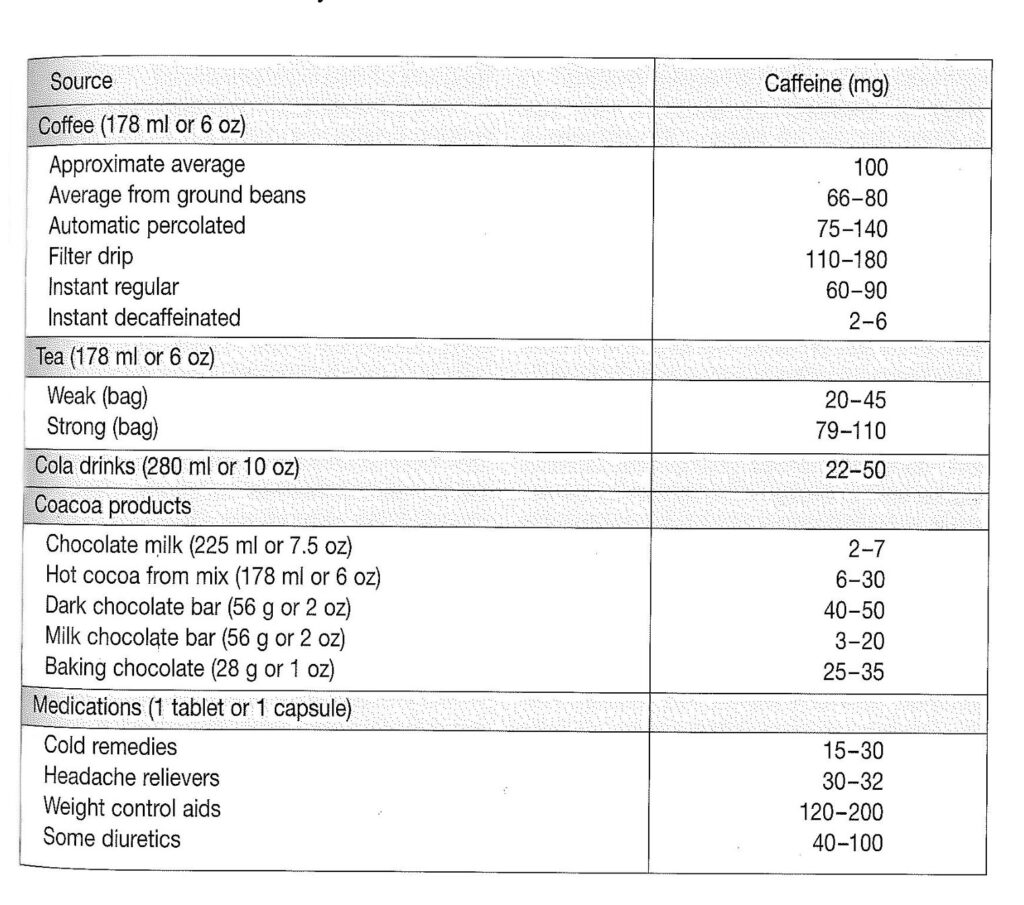
Table 6.5. Sources of caffeine. (From reference 48).
Based on these values the National Institute of Nutrition in Canada estimated that the average daily caffeine consumption of Canadians approximates 450mg per day. Children also consume large quantities of caffeine in the soft drinks and sweets which they consume, and this is a matter of some concern. Adults absorb 99% of the caffeine they consume, and peak blood levels are reached within 15-45 minutes, and the half-life of the caffeine (the time it takes to eliminate 50% of the caffeine from the system) varies from 3-7.5 hours. Caffeine is found in breast milk, and can cross the placenta and thus influence the unborn child. In newborn infants the rate of elimination of caffeine is much slower than in adults, and the half-life is 82 hours. In pre-term infants the half-life ranges from 62-102 hours.48 Some races also experience slower clearance rates than others, and Orientals have a much slower rate of elimination than Europeans. Pregnancy and the use of oral contraceptives also substantially increase the clearance rate.
The Federation of American Societies for Experimental Biology (FASEB) reported the mean consumption of caffeine to be 0.17 mg/kg per day for babies 0-11 months old, 0.49 mg/kg/day for age group 1-5 years, 0.31 mg/kg/day in the 6-11 year age group, 0.21 mg/kg/day in the 12-17 year age group and 0.18 mg/kg/day in the 18 year and older age group. In people with high consumption levels of soft drinks, levels can be significantly higher, and for children in the 1-5 year age group levels can reach 1.8mg/kg/day.49 In view of concerns about the safety of caffeine, and the relatively high concentrations to which children are exposed, the FDA has reviewed the use of caffeine as additives in soft drinks.
The effects of excessive caffeine intake, which in some individuals may be manifested at levels as low as 500 mg/day, include insomnia, headache, anxiety, irritability, and depression. When consumed on an empty stomach it can produce tremors, and at consumption rates of 1g (which is not unusual for some people) can produce symptoms such as fever, agitation, trembling, rapid breathing and heart rate, cardiac palpitations, diuresis, nausea and anorexia. Still higher intakes (5-100g or 50-100 cups of coffee) have caused tachycardia, convulsions, respiratory and heart failure and coma and death due to shock.48 People who stop drinking beverages containing caffeine may experience equally unpleasant withdrawal symptoms, the most common of which are muscle tension, nervousness, irritability and headaches. Caffeine also effects urinary calcium excretion, particularly in postmenopausal women.49 Rats fed instant coffee for 3 to 4 weeks also showed increased calcium loss via the urine and faeces.50 In one study carried out on a group of women (age 50-84), it was found that the consumption of more than two units of caffeinated beverages (one unit = one cup of coffee or two cups of tea), increased the risk of hip fracture by 69%.51 Metabolic studies have shown that the kidneys and intestinal system are directly affected by caffeine..
Of even greater concern than these immediate symptoms are the long-term dangers associated with caffeine, which can occur at lower levels and may be more subtle and difficult to detect. In studies on animals, caffeine was shown to affect the nervous system and influence such behaviours as learning, memory, motor performance, sensory function and emotional reactivity.52,53 These findings have prompted the FASEB to voice their concerns about behavioural effects of caffeine, and effects on the development of the nervous system in children who consume large amounts of cola-type beverages.
The administration of caffeine to pregnant mice indicates that caffeine has toxic effects on the unborn offspring and can possibly produce birth defects. Some of the birth defects noted after the administration of caffeine were: cleft palate, digital defects, muscular disorders, facial deformities, anophthalmia (absence of eyes) and exencephaly (the brain lying outside the skull). In rats the situation is similar, and incomplete ossification in the offspring was also reported.
As these studies suffered from lack of certain controls and low sample numbers the FDA undertook two new studies to resolve the issue of the teratogenic effects of caffeine. These studies revealed that high doses result in death and resorption of embryos, significant reductions in foetal weight, and skeletal abnormalities such as reduced pubis size, reduced dorsal arch and missing hind digits. In fact irreversible birth defects were noted at levels as low as 80 mg/kg and other defects at levels as low as 6 mg/kg.52 Much uncertainty still exists as to whether caffeine increases the risk of birth defects in humans, and it is premature to make such claims. Nevertheless, the studies on animals indicate that there are enough reasons for concern.
Alcohol and diet
It is an interesting phenomenon that many studies have shown that alcohol reduces the risk of coronary disease and may even have a positive influence on cholesterol levels.54 This phenomenon has received quite some attention and has given many an excuse for not curtailing their drinking habits. The negative aspects associated with alcohol, however, far outweigh any positive effects it may have on the cardiovascular system.55 Evidence is mounting that alcohol consumption increases the risk of cancer, particularly breast cancer, and although the relative risk is small (around 1.5), the alcohol habit is so widespread that it might account for a large proportion of breast cancers in Western countries.56,57
In a recent study, the effect of moderate intakes of alcohol on women 21 to 40 years old were assessed by measuring blood lipids at a time in the menstrual cycle when hormone levels were at their lowest. The subjects were given the typical US diet containing 36% fat and two 6-oz glasses of wine daily. Their total cholesterol levels remained unchanged, but there was an increase in HDL levels relative to LDL levels. This is indeed positive, but at the same time oestrogen levels rose from 7% to 37% during the menstrual cycle and this could be the reason why alcohol is associated with increased risk of breast cancer.58 Alcohol is probably not a direct carcinogen, but acetaldehyde, the main metabolic product in humans is a known carcinogen. Alcohol consumption is particularly linked with high risk of rectal cancer and the relative risks in individuals consuming three or more drinks per day were 3.17 (1.05-9.57).59 The IARC (International Agency for Research on Cancer) found that free extracts of some alcohol free beverages were also genotoxic, and the link between the consumption of alcoholic beverages, mainly beer, and rectal cancer was suggestive but not conclusive.59
Alcohol is known to impair the function of natural killer cells (NK) which destroy cancer cells.
Even small amounts of alcohol have a significant impact, and in one study it was found that just two cans of beer (3.5% alcohol) taken over a 30 minute interval during a meal significantly impaired the activity of lymphokine-activated killer cells (LAK) thus reducing the immune system’s capacity to clear virus infected cells or cell that have undergone neoplastic transformation. 60 It is sometimes claimed that alcohol contributes at least partially towards the overall nutrition, but alcoholic beverages provide little nutritive value apart from calories, and can not be equated with carbohydrates. Moreover, glucose homoeostasis is impaired by alcohol, and alcohol can affect insulin release and lead to glucose intolerance.61 Gout is also associated with alcohol, and short-term administration to patients, who have no disorders of renal function or uric acid metabolism, show significantly increased uric acid levels which persist, in some instances, for several days. Blood lipid levels are also raised by alcohol, and triglyceride levels can increase several-fold.62
It has been shown that alcohol is directly injurious to the small intestine and stomach. It can cause lesions in the duodenum and may impair the absorption of many nutrients.63 The liver is another organ that suffers from alcoholic intake and it has been shown that even daily alcohol consumption as low as 40g (± 3 drinks) in men and 20g (± 1½ drinks) in women resulted in a statistically significant increase in the incidence of cirrhosis in well-nourished persons.62 Vitamin metabolism is also impaired by alcohol, and reduction of liver stores of folacin, niacin, thiamin, vitamin B6 and vitamin B12 have been described. Fat-soluble vitamins are also negatively affected, and alcoholics have been found to have very low stores of vitamin A and vitamin D. Moreover, alcohol also results in greater renal losses of minerals, particularly zinc, calcium and magnesium, and the absorption of these minerals may also be impaired.62
A whole-food lifestyle, together with avoidance of harmful compounds, would circumvent many of the pitfalls associated with modern living. Whole foods will supply all the vitamins and minerals that the body requires to function normally, and at the same time most whole foods come prepacked in nature’s own wrappings. Many whole foods are naturally preserved, and fresh products allow one to largely avoid the many additives associated with processed foods. A diet consisting largely of fresh fruits, vegetables, grains, seeds, nuts and legumes can provide a whole new eating experience, and with a little bit of ingenuity will provide a satisfying alternative lifestyle.
REFERENCES
- Dwyer, J.T. 1988. Health aspects of vegetarian diets. Am.J.Clin.Nutr. 48:712-38.
- Position paper on food nutrition misinformation on selected topics. 1975. J.Am.Diet.Assoc. 66:277-280.
- Medeiros, D.M., Bock, M.A., Ortiz, M., Raab, C., Read, M. Schutz, H.G., Sheehan, E.T., Williams, D.K. 1989. Vitamin and mineral supplementation practices of adults in seven western states. J.Am.Diet.Assoc. 89:383-386.
- Read, M.H., Medeiros, D, Bendel, R., Bhalla, V., Harril, I., Mitchell, M., Schutz, H.G., Sheehan, E.T., Standal, B.R. 1986. Mineral supplementation practices of adults in seven western states. Nutr.Res. 6:375
- WHO. 1989. Global Nutrition Status Update. Geneva: WHO Publications, 1989.
- Scrimshaw, N.S. 1996. Nutrition and Health from Womb to Tomb. Nutrition Today, 31 (2) March/April pp.55-67.
- Ross, A.C. 1991. Vitamin A: Current understanding of the mechanism of action. Nutrition today. Jan./Feb. 1991, pp 6-12.
- Jacobs, C., Dwyer, J.T. 1988 Vegetarian children: appropriate and inappropriate diets.
Am.J.Clin.Nutr. 48:811-8.
- Johnston, P.K. 1988. Counselling the pregnant vegetarian. Am.J.Clin.Nutr. 48:901-5.
- Lindberg, A.S., Leklem, J.E., Miller, L.T. 1983. The effect of wheat bran on the bioavailability of vitamin B-6 in young men. J.Nutr. 113:2578-86.
- Reynolds, R.D. 1988. Bioavailability of vitamin B-6 from plant foods. Am.J.Clin.Nutr. 48:863-7.
- Callender, S.T., Spray, G.H. 1962. Latent pernicious anaemia. Br.J.Haematol. 8:230-40.
- Leitzmann, C. 1993. Vitamin B12 . Aktueller Stand der Forschung. Fit fürs Leben
6/93:12-15.
- Herbert, V. 1988. Vitamin B-12: plant sources, requirements, and assay. Am.J.Clin.Nutr. 48:852-8.
- Sherman, A.R. 1992. Zinc, copper, and iron nutriture and immunity. J.Nutr. 122:604-609.
- Hallberg, L., Rossander-Hulten, L. 1991. Iron requirements in menstruating women.
Am.J.Clin.Nutr. 54:1047-58.
- Greger, J.L. 1987. Mineral bioavailability / new concepts. Nutrition today. July/August 1987, pp 4-9.
- Kaneko, K., Masaki, U., Aikyo, M., Yabuki, K., Haga, A., Matabo, C., Sasaki, H., Koike,
G. 1990. Urinary calcium and calcium balance in young women affected by high protein diet of soy protein isolate and adding sulfur-containing amino acids and/or potassium. J.Nutr.Sci.Vitaminol. 36:105-116.
- Einhorn, T.A. Levine, B. Michel, P. 1990. Nutrition and bone. The Orthopaedic Clinics of North America. 21:43-50.
- Howe, J. 1990. Postprandial response of calcium metabolism in postmenopausal women to meals varying in protein level/source. Metabolism. 39:1246-1252.
- Blank, R.P., Diehl, H.A., Ballard, G.T., Melendwz,R.C. 1987. Calcium metabolism and osteoporotic ridge resorption: A protein connection. J. Prosthetic Dentistry. 58:590-595.
- Kitano,T., Esashi, T., Azami, S. 1988. Effect of protein intake on the mineral (calcium, magnesium, and phosphorus balance in Japanese males. J.Nutr.Sci.Vitaminol. 34:387-398.
- Greger, J.L. 1989. Effect of dietary protein and mineral on calcium and zinc utilization.
Critical Reviews in Food Science and Nutrition. 28:249-271.
- Godowski, P.J., Picard, D. 1989. Steroid Receptors. How to be both a receptor and a transcription factor. Biochemical Pharmacology. 38:3135-3143.
- Hunt, J.R., Johnson, L.K. 1992. Dietary protein, as egg albumen: Effects on bone composition, Zinc bioavailability and zinc requirements of rats, assessed by a modified broken-line model. Am.Inst.Nutr.122:161-169.
- Erdman, J.W., Garcia-Lopez, J.S., Sherman, A.R. 1987. Processing and fortification: how they affect mineral interactions? in Nutrition ’87, Levander, O.A., Ed., American Institute of Nutrition, Bethesda, MD.
- Murphy, E.W., Willis, B.W., Watt, B.K. 1975. Provisional tables on the zinc content of foods. J.Am.Diet.Assoc. 66:345-355.
- Kirk. R.S., Sawyer, R. 1991. Pearsons composition and analysis of foods. 9th. edition. Longman Scientific & Technical UK.
- Waslien, C.I., Rehwoldt, R.E. 1990. Micronutrients and antioxidants in processed foods – analysis of data from 1987 food additives survey. Nutrition today July/August 1990.
- Graham, D.M., Filer, L.J., Bigelow, S.W. 1990. Assessing dietary exposure to food additives: A new approach. Food Tech. July 1990, pp 94,96.
- Murdoch, R.D., lessof, M.H., Pollock, I., Young, E. 1987. Effects of food additives on leukocyte histamine release in normal and urticaria subjects. J. of the Royal College of Physicians of London. 21:251-256.
- Finegold, B.F. 1975. Why your child is hyperactive. Random House, New York.
- Weiss, B. 1983. The behavioral toxicity of food additives. Nutrition Update. Vol.1. Ed.
Weiniger, J. and Briggs, G.M. John Wiley & Sons, New York, pp. 21-38.
- Goyette, C.H., Conners, C.K., Pettit, T.A., Curtis, L.E. 1978. Effects of artificial colors on hyperkinetic children: A double blind challenge study. Psychopharmacol. Bull. 14:39
- Warrington, R.J., Sauder, P.J., McPhillips, S. 1986. Cell-mediated immune responses to artificial food additives in chronic urticaria. Clinical Allergy. 16:527-533.
- Schaubschl╠ger, W.W., Zabel, P., Schlaak, M. 1987. Tartrazine-induced histamine release from gastric mucosa. Lancet 39:800-801.
- Poulsen, E. 1991. Safety evaluation of substances consumed as technical ingredients (food additives). Food additives and contaminants. 8:125-134.
- Haigh, R. 1986. Safety and necessity of antioxidants: EEC approach. Food. Chem.Toxic. 24:1031.
- Tricker, A.R., Preussmann, R. 1990. Chemical food contaminants in the initiation of cancer. Proceeding of the Nutrition Society. 49:133-144.
- Kagan, V., Serbinova, E., Novikov, K., Ritov, V., Kozlov, Y., Stoytchev, T. 1986. Toxic and protective effects of antioxidants in biomembranes. Arch.Toxicol.Suppl. 9:302-305.
- Hemeda, H.M., Klein, B.P. 1990. Effects of naturally occurring antioxidants on peroxidase activity of vegetable extracts. J.Food Sci. 55:184-185,192.
- Olney, J.W. 1969. Brain lesions, obesity and other disturbances in mice treated with monosodium glutamate. Science. 164:719-721.
- Belluardo, N., Mudo, G., Bindoni, M. 1990. Effects of early destruction of the mouse arcuate nucleus by monosodium glutamate on the age-dependant natural killer activity. Brain Research. 534:225-233.
- Bloch, B., Ling, N., Benoit, R., Wehrenberg, W.B., Guillemin, R. 1984. Specific depletion of immunoreactive growth hormone-releasing factor by monosodium glutamate in rat median emminence. Nature. 307:272-273.
- Terry, L.C., Epelbaum, J., Martin, J.B. 1981. Monosodium glutamate: acute and chronic effects on the rhythmic growth hormone and prolactin secretion, and somatostatin in the undisturbed male rat. Brain Research. 217:129-142.
- Olney, J.W. 1971. Glutamate induced neuronal necrosis in the infant mouse hypothalamus.
J.Neuropath.Exp.Neurol. 30:75-90.
- Position statement on food labelling. American Institute of Nutrition and the American Society for Clinical Nutrition. 1990. Nutrient labeling of food products under consideration. Nutrition today. May/June 1990.
- Review from the National Institute of Nutrition in Canada. 1987. Caffeine: A perspective on current concerns. Nutrition Today. July/August 1987, pp 36-38.
- Massey, L.K., and S.J. Whiting. 1993. Caffeine, urinary calcium, calcium metabolism and bone. J.Nutr. 123:1611-1614.
- Jeh, J.K. and Aloia, J.F. 1986. Differential effect of caffeine administration on calcium and vitamin D metabolism in young and adult rats. J.Bone Minr. Res. 1:251-258.
- Kiel, P. Et al 1990. Caffeine and the risk of hip fracture: the Framingham study. Am. J. Epidemol. 132:675-684.
- Nightingale, S.L., Flamm, W.G. 1983. Caffeine and health. Current status. Nutrition Update. Vol.1. Ed. Weiniger, J. and Briggs, G.M. John Wiley & Sons, New York, pp. 3-19.
- Kirsh, K.R., Pinzone, M.G., Forde, J.H. 1974. Spontaneous locomotor activity changes evoked by caffeine in mice. Fed.Proc. 33:466.
- Rimm, E.B., Giovannucci, E.L., Willett, W.C., Colditz, G.A., Ascherio, A., Rosner, B., Stampfer, M.J. 1991. Prospective study of alcohol consumption and risk of coronary disease in men. Lancet 338:464-68.
- The Surgeon General’s Report on Nutrition and Health. 1988. DHSS publ. no. 88-50210.
Washington, DC: US Government Printing Office.
- Editorial, Hospital Update. 1991. Breast cancer and dietary factors. Hospital Update.
November 1991, pp 3-4.
- Graham, S. 1987. Alcohol and breast cancer. N.Engl.J.Med. 78:1211-1213.
- Clevidence, B. 1995. Alcohol and blood cholesterol. Nutrition Today July/August 1995. 30 (4) p 141.
- Bingham, S.A. 1996. Epidemiology and mechanisms relating diet to risk of colorectal cancer. Nutrition Research Reviews. (:197-239.
- Thylan. S. 1996. Soaking cells. New Scientist. 13 July 1996.
- Phillips, C.B., Safrit, H.F. 1971. Alcoholic diabetes: induction of glucose intolerance with alcohol. J.Am.Med.Assoc. 217:1513.
- Shaw, S., Lieber, C.S. 1983. Nutrition and alcohol: a clinical perspective. Nutrition Update. Vol.1. Ed. Weiniger, J. and Briggs, G.M. John Wiley & Sons, New York, pp. 79-104.
- Gottfried, E., Korsten, M.A., Lieber, C.S. 1978. Gastritis and duodenitis induced by alcohol: an endoscopic and histologic assessment. Am.J.Gastroenterol. 70:586.