To most people in the industrialized world a vegetarian lifestyle conjures up images of carrots and lettuce leaves, but nothing could be further from the truth. Vegetarian diets can be very satisfying indeed, as underscored by most of mankind that has subsisted for much of human history on vegetarian or near-vegetarian diets. Even in this modern age, the vast majority of the people who inhabit this planet subsist on a largely vegetarian diet.1 A prime example are the Hunzas of the Himalayas who are known for their disease-free society and longevity of life. The Tarahumara Indians of Mexico are also renowned for their stamina and vibrant health, yet both these tribes subsist on largely vegetarian whole-food diets.2 Vegetarian lifestyles are becoming more and more popular, and many people are adopting the vegetarian diet for reasons of health, religious beliefs, philosophical considerations or environmental convictions. However, not all the vegetarian practices dictated by some of these convictions are equally beneficial, and some of them, particularly those dictated by religious or metaphysical beliefs, can place severe restrictions on the utilization of certain foods. Moreover, some groups, in addition to following restrictive diets, shun the expertise of nutritional science and the medical profession, and run the risk of suffering malnutrition and associated diseases.
Vegetarians can be divided into various categories, depending on the range of foods which are included in the diet.
Vegan vegetarians: Avoid all animal products
Lacto vegetarians: Include dairy products in their diet
Lacto-ovo-vegetarians: Include dairy products and eggs in their diet
As discussed in the previous chapter, dairy products should, if possible, not be included in the human diet, and the other animal products also have their health risks, particularly in view of modern husbandry practices and the rising incidence of animal food-borne diseases. However, a diet that excludes all animal products might seem restrictive, and indeed can be, if certain criteria are not met. The more restrictive one’s diet the greater the chance of developing deficiencies and nutrient-deficiency related diseases. Risks will increase if single plant food regimes are adopted such as diets consisting only of fruit or only of legumes or only of cereals. The higher diet levels of the Zen macrobiotic diet are, for example, made up entirely of cereals, and cases of scurvy, anaemia, hypo-proteinaemia, hypo-calcaemia and even death from malnutrition have resulted from this lifestyle.3,4
Vegan vegetarian diets must be well planned, and special attention must be given to nutrients which occur in low levels or are absent from plant foods. Moreover, pregnant or lactating women and infants and growing children also need specific dietary consideration. However, if due consideration to these points is given, a total plant-based diet can supply all our dietary needs. At this point it can be emphasized again that a variety of plant foods, incorporating grains, nuts, seeds, legumes, fruits and vegetables, will supply ample nutrients for healthful living. Nutritionists often express scepticism as to the adequacy of a vegetarian diet, and their main concerns revolve around adequacy of proteins, calcium, iron, riboflavin and vitamin B-12.
If combinations of cereals and legumes are used, protein-deficiency is extremely unlikely, and numerous studies have proved not only the adequacy, but even the superiority of plant proteins over those of animal origin.3,5 Indeed, the reverse is true in that it is difficult not to exceed recommended protein allowances on a varied vegan diet. It is only when calorie needs are not met that the body will preferentially utilize proteins as an energy source, and this may result in
deficiencies. Such conditions are mostly found in populations where malnutrition is a common phenomenon. Regarding the other nutrients listed, all these nutrient requirements can be met by plant foods, except for vitamin B-12, but this can be supplied through fortified soybean milk, nutritional yeast grown on a B-12 medium, or through supplementation.6,7 Even without supplementation, reports of vegans suffering from vitamin B-12 deficiency are extremely rare (for a more detailed discussion of this issue, see chapter 6).
VEGAN DIETARY PRACTICES
Vegan diets in general are lower on calories than omnivorous diets, and as a result vegans are normally slimmer than their omnivorous counterparts. It was found that vegetarians weigh some 8kg less than meat eaters who in turn are, on average, 5-7 kg overweight.3 The lower weight of vegetarians has distinct health advantages in that slim people fall into lower risk categories regarding cardiovascular diseases and cancer.8,9 Obviously the body requires a minimum intake of energy to stay alive, and the number of calories required varies with sex, size and body weight. Adults require some 1 000-1 700 calories per day at rest (basal metabolic rate or BMR) whilst activity increases the energy expenditure. The average energy consumed per day is 2 000 calories for women and 2 700 for men, whereas heavy manual labour or sporting activity can increase the requirements to as much as 4 000 calories per day. The vegan diet has a lower fat and protein content and a higher carbohydrate content than most other diets, and particular attention must be paid to energy intake as the energy supply from fat is some 9,4 kcal/g, whereas carbohydrates and proteins supply only 4,2 and 4,3 kcal/g respectively.
Vegetarian dietary patterns for adults
Food guides in general are useful in teaching, but the average person will not pay much heed to them unless he can be educated to do so. The vegetarian tribes of the world also do extremely well without the use of dietary charts and lists of recommended daily allowances (RDA). The diets that have been established in these tribes have, however, arisen over time and have been practised for generations, whereas Western societies must rediscover simple wholesome eating practices. Moreover, there are so many so-called health foods and metaphysically inspired health notions, that the health-food industry has become a veritable minefield of misinformation. Under these circumstances it is prudent to make a thorough investigation of the issue, and not to avoid the voice of science.
In general the Western societies adhere to the Basic-Four nutritional guide which correlates adequate nutrition with regular intake of the four basic food types: Dairy products, breads and cereals, fruits and vegetables and meat. It is interesting that even this Basic-Four Food Guide was found to be lacking in vitamin E, vitamin B-6, magnesium, zinc and iron.10 In the past, these four food groups were depicted as of equal importance, and the plate was divided into four quarters each with one of these food groups. This Basic-Four diet has recently come under attack from health circles, but intensive lobbying by the meat and dairy industry have managed to keep it at least partially afloat in the minds of the general public. In the past American school children were taught that a healthy diet included meat every day, but now the US government has recognised that a vegetarian diet can be healthy. In 1992 the USDA issued a revised recommendation in which the “food pyramid” was used for the first time. It was now suggested that grains and cereals form the bulk of the diet, vegetables and fruits were suggested as next in importance followed by animal product and finally fats, oils and sugars which were to be used sparingly. The 1996 guidelines are a further advance on this, and the
inclusion of vegetarianism as a healthy alternative may almost be considered bold. The 1996 guidelines state “ Most vegetarians eat dairy products and eggs and, as a group, these lacto-ovo-vegetarians enjoy excellent health”. The guidelines, however still warn against a strict vegan diet and supplementation of iron, zinc, and B-vitamins is suggested.11 The change of heart comes from an overwhelming body of evidence that the consumption of animal products is a health risk, and it can be expected that more changes in lifestyle will be recommended in the future. Already, Michael Jacobson, executive director of the “Centre for Science in the Public Interest” criticized the US government for not coming out more strongly against meat in the 1996 guidelines.11 Vegan vegetarians need different guidelines to those commonly accepted in Western societies, and they need to plan their eating regimes carefully, nevertheless a balanced vegan lifestyle is not only possible, but can indeed be desirable in terms of health.
Ovo-lacto- and lacto-vegetarians have less of a problem in meeting caloric needs than do vegan vegetarians, and that is why the safety of lacto-ovo-vegetarian eating patterns is normally emphasized in dietetic recommendations, whilst specialized dietary planning is recommended for vegan type diets.6,12 The energy component of ovo-lacto-vegetarian diets is boosted by the animal fats included in these diets and are therefore not to be regarded as a positive aspect of these diets. Vegan vegetarians must plan diets that will compensate for the omission of dairy products, by ensuring that they include adequate quantities of high energy foods in their diets, which must also meet all the other basic needs of the body. Provided this is done, it has been shown that a vegan diet can provide all the body’s needs and can be followed without fear. A number of suggested vegan diet patterns have been analysed, and it was found that the diet suggested by Selma Chaij-Rhys came closest to satisfying daily nutritional needs of adults.7,16 In addition this diet uses a simple numerical formula and starts off by using grains, fruits, nuts and vegetables, and adds vegetable-protein foods fortified with vitamin B-12, such as fortified soy milk or simply a B-12 supplement. The numerical formula used in this diet guide is the 1-2-3-4-5 pattern, to help the user remember the number of servings to be used in each food category per day (Table 5.1).

Table 5.1. Chaij-Rhys diet plan for adult vegans. (From ref. 6 and 13)
This eating pattern will supply more than double the RDA of iron, particularly as the high vitamin C content will enhance the utilization and absorption of non-haem iron.14 Riboflavin and niacin needs are also met. The pattern, however, falls short in protein and energy, particularly in men, but the use of a larger serving size would help to bridge the energy gap. In women the Chaij-Rhys diet plan will supply adequate nutrition in all the nutrients with the exception of calories. Again a somewhat larger serving will cater for all the needs, including energy needs.
To satisfy protein needs, correct food combinations are essential, as various plant-protein sources complement one another. This issue will be discussed more fully in chapter 7, but an example can be given here to illustrate the point. Legumes are high in lysine but low in the sulphur-containing amino acids methionine and cystine, and the combination of legumes with grains, which are high in methionine and threonine and low in lysine, will provide an excellent protein.15 To achieve a proper amino-acid balance is thus not nearly as complicated as it sounds, and the ordinary peanut butter sandwich will supply complete proteins as it is a combination of a grain (wheat) and a legume (peanuts).
Dietary patterns for pregnant and lactating mothers
Vegetarian women are on the whole more health-conscious than non-vegetarians and will tend to adjust their diets to meet the demands of pregnancy or lactation. Pregnant women have greater energy needs, but the relative increase in energy needs is small compared to the greater need for certain vitamins and minerals (Fig. 5.1).

Figure 5.1. Percent increase in dietary needs during pregnancy. (From reference 15)
This data suggests that the choice of energy-rich foods during pregnancy must also include adequate concentrations of vitamins and minerals. Nutrients that need particular attention during this period are vitamins D and B-12, calcium, iron and zinc. Fortified soy milk is a good way of obtaining these nutrients, particularly B-12, as deficiencies of this vitamin have been reported in cases of breast-fed infants whose mothers were vegans.17
Dietary patterns that supply satisfactory quantities of nutrients for pregnant women are the Seventh-day Adventist Dietetic Association plan for pregnant women.6 This plan requires four protein servings of nuts, seeds or legumes, four soy milk servings, six grain or cereal servings, and eight servings of vegetables or fruits per day.18 The Chaij-Rhys plan does not supply sufficient nutrients to cater for the increased demands of pregnancy, even if an additional serving is added in each category of food,6 but if more fortified soy milk is added in addition to the increased number of servings, then nutrient levels should satisfy the additional demands experienced during pregnancy or lactation. In countries where fortified soy products such as soy milk are not readily available it is advisable to take supplements or to add vitamin D and B-12 to home-made soy milk.
Finally it is strongly recommended that one minimizes the use of empty-calorie foods such as refined foods, and concentrate on whole foods. Additionally, it goes without saying that substances and foods that are detrimental to health, such as alcohol, tea and coffee, should be avoided at all costs during pregnancy.
Dietary patterns for infants and young children
Children have smaller stomachs than adults and they have higher needs for nutrients per unit weight, therefore diets that are appropriate for adults can indeed be deficient for young children. Children under three years can accommodate only 200-300ml food at each meal, and a high-fibre, low-calorie diet will put them at risk in view of their inability to consume sufficient quantities to meet their needs. Restrictive dietary regimes should again be avoided, and there must be a shift to more high-energy foods in order to sustain normal development. Again, variety is the watchword, and single-plant food diets, such as an exclusively fruitarian diet, would not supply sufficient nutrients for normal development.
Mother’s milk is the best food there is for infants. It is not advisable, if it can be helped, to substitute mother’s milk for the milk of other animals, as the composition of milk varies from species to species. Human infants are designed to drink human milk and a demand-type breast-feeding schedule would go a long way in meeting the infants’ needs, failing this, one should ensure that infants consume adequate quantities per meal as dictated by their age. The composition of mother’s milk will also vary with the mother’s diet, but it can be said that good wholesome food will make good wholesome milk. On the whole, the breast milk of vegetarians contains fewer environmental contaminants and additives than does the milk from omnivores,19 and it has been found that the vegetarian infant can thrive if care is taken to supplement iron, B-12 and vitamin D intake.
When the transition from breast-feeding to table foods is made, care must again be exercised not to follow restrictive diets as followed by some groups such as Zen macrobiotics, Black Hebrews and Rastafarians. These diets are normally schooled around a few grains, vegetables and fruits in addition to milk made from grains. They are often deficient in calories and proteins as well as numerous minerals and vitamins, particularly vitamins D and B-12. Such diets have led to numerous hospitalizations for malnutrition, and have been responsible for the deaths of a number of children.15,20,21
Some grains such as maize, increase up to six times in volume when cooked as a porridge, thus drastically reducing the energy content per unit-volume. Porridges in general will not supply sufficient energy for small children, and increased intake of cereals, nut butters, avocados, dried fruit spreads and legumes is recommended whilst limiting the amounts of fruits, vegetables and porridges (gruels).15,22,23 Nut butters such as almond, brazil, cashew, peanut, pecan and walnut butters or sesame-chick-pea butter, can be given to toddlers whilst avocado can also be served even to infants.22 Avocados are a rich source of numerous nutrients including fat, copper, potassium and riboflavin, and in view of their fat content they also supply more energy per unit mass than other fruits. Care must also be taken to choose combinations of grains and legumes or nuts and seeds to satisfy the amino acid requirements of vegan children. Furthermore, weaned children should receive vit. D and B-12 fortified soy milk or nut milk, particularly in areas where exposure to the sun is limited. Bearing these points in mind, it has been shown that vegan diets can support normal growth and development.24 In table 5.2 a diet plan for young vegan children is presented.

Table 5.2 Diet plan for young vegan children. (From reference 22).
The nutritive value of the diet plan for vegan children supplies sufficient nutrients to meet the demands of growing children, and can be substantially increased by more liberal servings. The nutritive value of the above diet plan is presented in figure 5.2.
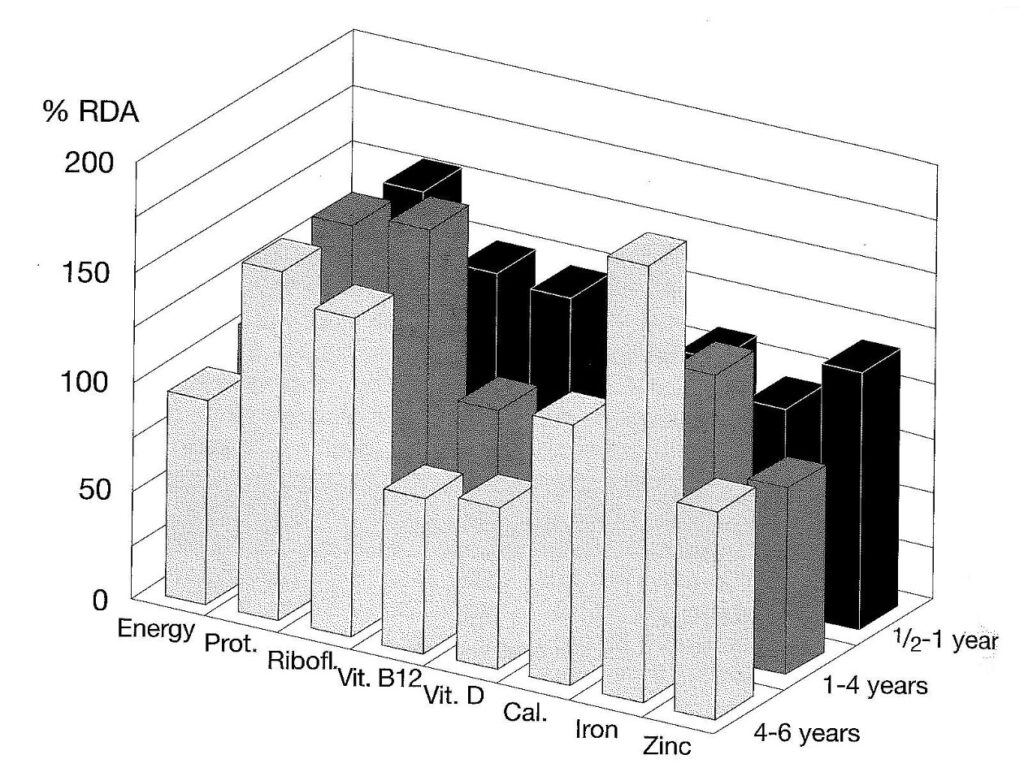
Figure. 5.2. Nutritive value of the basic diet plan for vegan children. Energy content can be increased with more liberal servings, B12 content can be improved by increased supplementation, vit. D by exposure to sunlight or supplementation and zinc content by the addition of wheat germ or supplementation. (From reference. 22)
As stomach capacity increases a gradual shift to adult eating patterns can take place. Preschoolers should still receive greater portions of energy-rich foods and foods high in Ca, Zn, Fe, plus supplementation of vitamin D and B-12.25 Furthermore, it is important to ensure a good mix of plant-protein sources. A whole-food diet, comprising legumes, grains, nuts, seeds, fruits and vegetables (inclusive of the leafy green varieties) together with fortified soy milk will have children brimming with health. If wholesome eating practices have been adopted in the family and care is taken to supply the special needs of younger children, then there is no need for concern. Furthermore, it is not necessary to cook separate meals for younger children, but merely to ensure that the relative portions that children obtain are geared to their needs.
Parents tend to enforce their own eating habits onto their children and might insist that the child eat more of the vegetables or fruits than of the nut-grain-legume dishes which the child needs for growth. Moreover, children also have a natural tendency to consume more of the energy-rich foods, and this should not be discouraged as long as it does not lead to the exclusion of the other essential foods. Healthful eating patterns should be established early, and if parents are concerned about the health and well being of their vegan children, then a “do as you please” attitude should not be adopted. However, having said this, it is also important that flexibility should be maintained and extremes avoided. Eating should be a pleasure, not a burden, and mealtimes should be something to look forward to. There should be a relaxed atmosphere at the table, conducive to good digestion, and children should not feel pressurized because parents hold very rigid, or fanatical views on nutrition.
A study done on British vegan children showed that the average energy intake was less than the recommended daily allowance for British children in general, particularly in the 2-4 year age group. But this is not uncommon, as many non-vegetarian children fail to meet the RDA. The average nutrient density, however, was higher for vegan diets for most nutrients, with the exception of calcium and fat, when compared to the average UK diet. The children tended to be lighter than the average, but normal in terms of their blood formation, educational and physical development. Vegan diets have received a bad press because of a few inappropriate diets, but appropriate vegan diets will rear healthy children. Moreover, there is no evidence that either intellectual function or physical stamina are adversely affected by a well-planned vegan diet.24
Adolescents and young adults
Adolescents have greater needs for energy, protein, Ca, P, Fe, Zn and vitamin A because of the rapid growth during this stage.15 Besides catering for the higher protein and energy needs, care should be taken that the diet includes green leafy vegetables or other foods rich in calcium. Supplementation to augment supplies of B-12 and zinc are also recommended for this stage.
Energy requirements
Energy requirements depend largely on lifestyle, but tend to vary between 1 800 calories per day for a sedentary to mildly active individual to in excess of 3 500 calories per day for intensely active individuals. Vegan vegetarians need to consume a greater proportion of high energy foods such as grains, legumes, seeds, nuts and energy rich fruits and vegetables than do non-vegans. Non-vegan vegetarians tend to have a higher fat intake than vegans, because of the consumption of dairy product and eggs, and this makes it easier for them to meet their energy demands. The consumption of these animal fats and proteins, however puts them in a higher risk category in terms of degenerative diseases. Normally, the natural cravings of the system will ensure that sufficient energy-rich foods are consumed, particularly by active people, but when there are changes in lifestyle it may be useful to calculate what the body’s needs are in order to put one’s mind at rest.
To calculate the daily number of calories required for one’s particular lifestyle, it is necessary to know what one’s BMR (Basal Metabolic Rate) is, and the multiple of BMR associated with a particular lifestyle. The BMR is the energy expended while lying awake but completely still and the multiple of BMR is the factor by which BMR must be multiplied in order to account for other daily activities such as walking etc. The “Dunn Clinical Nutrition Centre” in Cambridge UK, recently collated measurements from all over the world in order to estimate the multiple of BMR associated with various activities. These are summarised in table 5.3., and the formulas for calculating the BMR are presented in table 5.4.

Table 5.3. The multiple of BMR associated with various activities.( From reference 26)

Table 5.4. Equations for calculating BMR. (From reference 26)
Using the data above, it is now possible to calculate the total energy needs per day. First calculate the BMR using the formulae in table 5.5 and multiply it by the appropriate “multiple of BMR” from table 5.4.
Example:
A housewife aged 35 and weighing 55 kilograms
BMR = (8.3 x 55) + 846 = 1302
Multiple of BMR for a housewife = 1.8
Total calories required = 1302 x 1.8 = 2345
To convert to kilojoules, multiply this figure by 4.2
HEALTH ASPECTS OF THE VEGETARIAN DIET
Vegetarians have a lower incidence of degenerative diseases than do non-vegetarians, and as the foundations for many of these diseases are already laid in childhood,27 it is prudent to establish good eating habits early on in life.
The vegetarian lifestyle has often been met with suspicion, if not outright scorn, but in recent times the positive effects of a vegetarian lifestyle have come to be recognized. More research has been done on vegetarianism in the past two decades than in the entire history of the human race, and thorough reviews of the relevant literature exist.28 Of all the vegetarian groups studied, the World Health Organization made special mention of the Seventh-day Adventists as they, on different occasions have received special notice because of their low number of heart attacks, cancer and other diseases related to lifestyle.29 Seventh-day Adventists generally, though not exclusively, follow a vegetarian lifestyle, with all types of vegetarianism represented. They also avoid alcohol and smoking, which makes them an ideal study group and probably accounts for the fact that mortality rates for lung cancer are only 20% of those of the general populace, whereas the low figures for throat cancer (5%), bladder cancer (28%) and cirrhosis of the liver (13%) are probably also as a consequence of the avoidance of these commodities. Mortality is also down for most other diseases, and with the exception of breast cancer (72%), digestive tract cancer (65%), ovarian cancer (61%) and heart attacks and angina
(55%), the mortality for most other diseases is less than 50% of that of the general populace.5,28,30,31,32,33,34,35,36
In view of the strong correlation between the consumption of dairy products and eggs with some of the types of cancers listed above, it is not surprising, that those who’s lifestyles where more vegetarian, or tended towards the vegan lifestyle, had lower age specific mortality rates than those whose lifestyles tended towards omnivorous diets.37 Numerous studies, on vegetarianism in general, have shown that it is not only the longevity of life that is extended in vegetarians, but that the quality of life is also improved. This is because many of the common diseases that plague mankind are less prevalent among vegetarians than among their omnivorous counterparts.
Vegetarianism and obesity
The body mass of vegetarians in general, and vegans in particular, is closer to the desirable level than the body mass of non-vegetarians.37 People with a body mass 20% above optimal are considered to be at a significantly greater risk of mortality or morbidity (contracting a degenerative disease) than people with normal, or slightly under normal weights.38 The level of obesity can also be assessed by measuring the waistline. A measure of more than 35 inches (78,9 cm) for women and 40 inches (101,6 cm) for men indicates obesity. As percentage overweight is not the easiest parameter to work with, and waistline measurements can be arbitrary, obesity is usually expressed in terms of body mass index (BMI). Clinical obesity is defined as a BMI which is greater than 30. Desirable BMI would be in the range 20 -25. BMI can be calculated as follows:

Obesity is on the increase in affluent societies, and can be ascribed to changes in lifestyle. The reasons for obesity are multifactorial, but increased consumption of fatty foods, overeating and more sedentary lifestyles are the main reasons sited for this phenomenon. Since the last world war, the British population has shown an increase of 3 BMI units in weight and the average adult is now 10 kg heavier at an equivalent height than five decades ago. Since the mid 1980’s, the number of clinically obese people has doubled in the UK,39 and figures for the USA are similar, with 33.4% of the adult population being obese and one in ten 12- to 19-year olds are significantly overweight.40,41 The changes fat consumption relative to carbohydrate consumption in the UK are presented in figure 5.3.)

Figure 5.3. Changes in carbohydrate and fat incorporation in the diet over time in the UK. (From references 39).
Studies have shown, that a high fat-carbohydrate ratio in the diet is associated with obesity.42 The old notion that overweight people should cut down on carbohydrates is thus not true, they should cut down on fat in the diet. In fact, data compiled from over 11 600 Scottish men and women showed that the groups consuming the most sugar had the lowest level of obesity, and this can be ascribed to the lower fat intake associated with a high carbohydrate intake.39 However, not all people on a high fat diet become obese, and there must be other reasons as well as to why some are more prone than others to becoming obese. Nevertheless, a reduction in fat consumption can lead to the desired weight loss in obese people without undue restrictions in the amount of food consumed. It the change in the ratio of fats to carbohydrates that induces the weight loss. Studies on the effect of reduced fat diets have shown that if the percentage fat in the diet is reduced to between 15% and 20% then weight loss follows in obese people even if their overall consumption remains the same.39
Obese people are up to three times more likely to die prematurely than lean people, and the most likely conditions from which they may suffer are heart attacks, strokes, and some forms of cancer. Many studies have shown that obesity is associated with increased risk of hypertension, insulin resistance and diabetes, hypertriglyceridaemia reduction in the levels of HDL-cholesterol and increases in the levels of LDL-cholesterol as well as other diseases such as gout, gallstones, renal failure, infertility and degenerative joint diseases such as arthritis. Moreover, Obese individuals also tend to suffer more frequently from
psychological problems and depression. Obese women are at a greater risk of contracting endometrial cancer, whereas in obese men the risk of prostate cancer is increased.38 In fact the risk of cancer in general is increased, and the incidence of breast, colon, rectum, kidney, cervix, ovary, thyroid and gallbladder cancer is higher in obese than in normal people.43 The issue is however complex, as fat intake and detrimental habits such as smoking and drinking cloud the issue. A study on 750 000 men and women showed that the effect of obesity seems to differ between the sexes. Men who are within 10% of their ideal body mass had the lowest risk of contracting colon, prostate and kidney cancers, whereas women who were 10-20% below the average weight for age and height had lower incidences of colon, breast, uterus, gallbladder, ovary, cervix and kidney cancer.44
The distribution of body fat is also significant in determining the level of risk. Abdominal obesity is more dangerous than gluteal-femoral (upper thigh and buttocks or pear-shaped) obesity. In women the effect of an increased Waist-to-hip ratio (commonly referred to as apple-shaped) has been positively linked to cancer. Increased levels of upper body or abdominal fat have also been related to hypertension and diabetes. Moreover, in some cases it seems probable that the distribution of body fat is of greater significance in increasing the risk of disease, than is the degree of obesity.38
Adipose tissue increases the levels of oestrogens, and increased levels of these hormones have been associated with cancer, particularly of the breast. Pre-menopausal women who are vegans or are on a low-fat vegetarian diet, have lower levels of oestrogens and their menstrual cycles are also shorter by 1-2 days.45 Western diets lead to raised levels of oestrogen in general and this has been associated with cancer. Breast cancer rates are lower in countries where vegetarian diets are commonly consumed.28 The issue is complex, and the causes of cancer are multifactorial. Nevertheless, it has been established that a vegetarian diet offers protection against specific cancers, and colon cancer rates in vegetarians are lower than in non-vegetarians.46 Secondary bile acids have been linked to intestinal tumour formation, and here again vegan vegetarians have the lowest ratio of secondary to primary bile acids.47 Furthermore, cell proliferation, a factor correlated with tumour growths and development,48 is lowest in the colon of vegetarians.28
The dangers of undernutrition
The Body Mass Index (BMI), is the most convenient indicator of chronic undernutrition. As noted previously, a desirable BMI would be in the range 20 -25, but low BMI values also impact negatively on health. In India, individuals with a BMI lower than 16 had a mortality rate of 32.3/1000/year compared with 12.1/1000/year in individuals with a BMI greater than 18.5. Figure 5.4 shows the relationship between low BMI’s and fathers not working because of illness. Women suffer even more than men in this regard.

Figure 5.4. Relationship between BMI and fathers not working due to illness in Bangladesh. (Adapted from references 49 and 50)
Whilst it is true, that high fat intakes can lead to obesity, fat intake should be regulated to maintain a desirable BMI. Moreover, fat intakes that are desirable for adults may be totally inappropriate for infants and growing children. Fears that fat consumption in children may lay the foundation for cardiovascular disease, cancer and other degenerative diseases in adulthood, may have been premature, as there is no convincing scientific data to support this claim. The fact is, children need more fat in their diets than adults.51,52 Vegan vegetarians on a whole food low fat diet should monitor their children to ensure that they receive adequate quantities of fat in the diet. This can be achieved by selecting whole foods with a high fat content such as nuts, seeds, avocado, olives and high fat legumes. Spreads and nut or seed creams and milk can be used liberally by children whereas adults may need to restrict the intake of large quantities of these foods. The key lies in monitoring ones BMI, and using foods with a high fat content to maintain body weight at an optimum. Children on vegan diets need not and should not look like undernourished children.
At a recent symposium of the American Institute of Nutrition, the following point of view found substantive support: 1) Providing adequate energy and nutrients to ensure adequate growth and development remains the most important consideration in the nutrition of children.
2) During preschool and childhood years, nutritious food choices should not be eliminated or restricted because of fat content. During early adolescence, and energy intake adequate to sustain growth should be emphasised, with gradual lowering of fat intake. Once linear growth has stopped, fat intake at the level recommended for adults is appropriate. 3) Food patterns that emphasise variety and complex carbohydrates and include low-fat choices are appropriate for children. 4) Physical activity and healthy eating are important lifestyle habits for children. They conclude that from the age of two until the end of linear growth there should be a transition from the high-fat diet of infancy to one with no more than 30% of calories from fat and no more than 10% of energy from saturated fat.52
Diabetes mellitus
Diabetes has two forms: Insulin Dependant Diabetes or Type I diabetes which normally develops early on in life as a consequence of the destruction of insulin-producing cells in the pancreas. Non-Insulin Dependant Diabetes or Type II diabetes which usually develops later on in life. In Type II diabetes, the pancreas produces insulin, but production is impaired. This disease is positively correlated with lifestyle and obesity in particular. Individuals with a BMI of 30 are seven times more likely to develop Type II diabetes than are non-obese people. Individuals with a BMI of 42 have 42 fold increase in risk (Figure 5.5).53

Figure 5.5. Increase in relative risk of contracting diabetes with increase in BMI. (Adapted from ref. 53.)
Diabetes mellitus is another disease that occurs less frequently among vegetarians than among non-vegetarians. An American study showed that Seventh-day Adventists (who follow mainly a vegetarian lifestyle) are only half as likely to develop this disease than the American population as a whole.54 The fact that vegetarians in general consume more complex carbohydrates in the form of whole foods, and thus have a more gradual release of glucose from the intestinal tract, is one of the factors which affords protection against hyperinsulinism and glucose surge associated with a diet of refined foods. Vegetarians, and vegan vegetarians in particular are less likely to be obese, and this affords further protection, particularly, since a Scandinavian study showed that even moderate obesity was associated with a 10-fold rise in the risk of diabetes, and this risk increased substantially with more severe obesity.38,55
Cardiovascular disease
The evidence that vegetarians have lower blood pressures than non-vegetarians is impressive. This is even true if the non-vegetarian group consist of non-smokers, though abstinence from alcohol may also help to keep the blood pressures of vegetarians lower than that of non-vegetarians.56 The increase in blood pressure with age is also significantly less in vegetarians than in non-vegetarians. Furthermore, blood pressures of vegan vegetarians are slightly lower than those of ovo-lacto vegetarians, being some 5-8mm Hg lower in the vegans.57 When 250 g/day of lean beef was fed to 21 strict vegetarians it was found that systolic blood pressure increased significantly by the third week, but diastolic blood pressure was not significantly affected. Furthermore, plasma cholesterol levels rose by 19% during the meat period but returned to normal after ten days on the vegetarian diet.57 It has been shown that increase in blood pressure cannot be attributed to the presence of meat protein, so some other factor must be responsible for the observed blood pressures of vegetarians.58 Considering that even a small reduction in systolic blood pressure (5 mm Hg) can substantially reduce the number of major coronary events, it is not surprising that vegetarians are less likely to suffer heart attacks, resulting from cardiovascular disease, than their omnivorous counterparts.37,59 In figure 5.6 a typical blood pressure profile of vegetarians and non-vegetarians is shown.

Figure 5.6. Blood pressure in vegetarians (squares) and omnivores (dots). Results of systolic and diastolic pressures for men are shown on the left and those for women on the right. Adapted from reference 59).
Osteoporosis
Calcium loss from bone causes osteoporosis which is particularly prevalent in postmenopausal women. In a comparative study between 1 600 ovo-lacto-vegetarians and omnivorous women in Michigan USA it was found that the vegetarians had only 18% loss of bone mineral by age 80, whereas closely paired omnivores had 35% loss of bone mineral.60 High-protein diets cause calcium loss in the urine,61 and evidence suggests that the rates of osteoporosis are higher in Western countries than in developing countries where diets tend to be vegetarian. The higher rate of calcium excretion may also be a reason for the observed higher incidence of kidney stones in affluent Western societies than in vegetarian or semi-vegetarian societies.
In a study carried out on merino rams, in which fifty weaned (100 day old) rams were divided into five groups of ten and fed diets containing either 20% plant protein (gluten-grain) or a mixed ration consisting of 12% plant and 8% animal protein (fishmeal and bloodmeal as is standard practice in the animal husbandry industry) it was shown that the addition of animal protein to the diet severely compromised bone development, although weight gain and food consumption did not differ significantly between the two groups.,62,63,64 Increased protein consumption enhanced calciuresis and resulted in significant limb skewness. The limb skewness could not be ascribed to osteopenic bones and compared with animals consuming lower protein rations, the bone mineral density (BMD) and vertebral trabecular bone volume (TBV) of animals fed high protein diets were significantly increased. In animals consuming higher protein diets, skeletal radiology and quantitative bone histology revealed no evidence of bone turnover as would be expected in animals which are in negative calcium balance. The ratio of Calcium:Phosphorus in the bone was inversely correlated with increased protein intake and resulted from an increase in phosphorus content of bone while the amount of bone calcium was unaffected. Bone density was thus not a good indicator of bone strength, as sheep with the highest BMD were worst affected by limb deformity.
A comparison between those sheep receiving the highest protein rations (20% plant protein vs. 20% protein of which 12% was of plant origin and 8% of animal origin) showed that the addition of animal protein significantly impaired bone development. The group receiving animal protein showed a significant increase in calciuresis (figure 5.7 a), had a higher BMD (fig.5.7b), increased limb deformity (fig. 5.7c) and had a lower calcium to phosphorus ratio (fig. 5.7d) than those receiving plant proteins. This study shows, that the common practice of measuring BMD as an indicator of bone strength and the risk in terms of osteoporosis, is not necessarily sound. Other factors, such as qualitative micro-architectural abnormalities, and not mere bone loss, may underlie the skeletal deformities induced by increased protein consumption, particularly animal proteins.

Figure 5.7. Change in parameters reflecting bone mineral status in merino rams fed diets containing only plant proteins (20% plant protein) and mixed proteins (12% plant and 8% animal). Units for deformity are arbitrary units in which 50 represents normal straight legs and 100 would represents legs bent at a 90° angle. (From reference 64).
Preliminary results in follow up studies on rats, rabbits and vervet monkeys, using the milk protein casein as animal protein source, and comparing it with plant protein (soya), show the same trend in all the groups studied. In our modern society the notion exists that dairy products are essential for maintenance of calcium levels and prevention of osteoporosis. Vegan diets are often criticized on the grounds that they will lead to severe calcium depletion. In fact there is no evidence that this is the case and if anything, the reverse is true, as indicated by current research findings. Moreover, osteoporosis is more prevalent in Western countries where an abundance of milk is consumed than in countries where vegan diets are more common.28 There is also no clear evidence that dietary calcium supplementation will slow the rate of bone loss in postmenopausal women, a position also held by the US department of Health and Human services.65
Rheumatoid arthritis
Obesity once again plays a role in the prevalence of this disease, and vegetarians in general are advantaged over non-vegetarians in that they tend to have lower body masses. Many claims have been made that vegetarian diets will cure arthritis, but these claims could not be readily substantiated.28 It is known that most patients with rheumatoid arthritis benefit from a short period of fasting, but in most cases there is a relapse as soon as food is reintroduced. However, a recent study showed that a vegan diet, which also excluded citrus fruit, salt, refined sugar, strong spices, tea, coffee and alcohol substantially reduced the negative symptoms of this debilitating disease, and this improvement was maintained even if the patients were gradually reintroduced to dairy products.66 The change from an omnivorous to a vegetarian diet causes a considerable change in the fatty-acid profile of the serum phospholipids,67 and these changes can stimulate the production of prostaglandins and leukotrines, which can counteract inflammatory activity.
At this point a word of admonition might be in order. The vegetarian life-style is not to be regarded as an instant cure for all the ills that prevail in industrialized societies. Unfortunately, some over-enthusiastic groups have made such claims in the past, and the impression is created that the vegetarian lifestyle is not only an alternative lifestyle, but a substitute for commonly accepted medical norms. Nevertheless, from the evidence it is clear that the vegetarian lifestyle offers a healthy, satisfying alternative to the commonly accepted diet of the industrialized world. Moreover, a number of studies have shown that properly conducted vegetarian diets, including vegan diets, fare well when they are compared in terms of their adequacy of nutrients, to non-vegetarian diets.68 What is more, these diets were found to be exemplary and, more in line with dietary recommendations than were diets of omnivores.
In closing it is important to remember that variety should be the watchword in any vegetarian diet, and if the simple rules are adhered to then one can adopt this lifestyle with complete peace of mind.
REFERENCES
- American Dietetic Association. 1980. Position paper on the vegetarian approach to eating.
Am.Diet.Assoc. 77:61-69.
- Balke, B.; Snow, C. 1965. Anthropological and physiological observations on Tarahumara endurance runners. A.J.Phys. Anthropol. 23: 293-301.
- Register, U.D. and Sonnenberg, L.M. 1973. The vegetarian diet. J.Am.Diet.Assoc. 62: 253-261.
- Council on Foods and Nutrition. 1971. Zen Macrobiotic diets. J.A.M.A. 218:397.
- Snowdon, D.A. 1988. Animal product consumption and mortality of all causes combined, coronary heart disease, stroke, diabetes and cancer in Seventh-day Adventists. Am. J. Clin. Nutr. 48: 739-48.
- Mutch, P.B. 1988. Food guides for the vegetarian. Am. J. Clin. Nutr. 48:913-9.
- Nieman, D.C. 1988. Vegetarian dietary practices and endurance performance.
Am.J.Clin.Nutr. 48: 754-61.
- Beil, L. 1988. Lean living. Science News 134: 142-143.
- Butrum, R.R., Clifford, C.K., Lanza, E. 1988. NCl dietary guidelines: rationale. Am. J. Clin. Nutr. 48: 888-95.
- King, J.L., Cohenour, S.H., Corruccini, C.G. Schneeman, P. 1978. Evaluation and modification of the Basic Four Food Guide. J.Nutr.Educ. 10:27-9.
- Kleiner, K. 1996. Life liberty and the pursuit of vegetables. New Scientist. 13 January, 1996
- Michigan Department of Public Health. 1980. Basic Nutrition facts. Lansing, M.I.: MD PH (MDPH publication) H-808.
- Chaij-Rhys, S. 1980. A diet pattern for total vegetarians. Adventist Rev. 157: 1014-4.
- Smith, M.V. 1988. Development of a quick reference guide to accommodate vegetarianism in diet therapy for multiple disease conditions. Am.J.Clin.Nutr. 48;906-9.
- Jacobs, C. and Dwyer, J.T. 1988. Vegetarian children appropriate and inappropriate diets.
Am.J.Clin.Nutr. 48:811-8.
- Johnston., P.K., 1988. Counseling the pregnant vegetarians. Am.J.Clin.Nutr.é48:901-5.
- Davis, J.R., Goldenring, J, Lubin, B.H. 1981. Nutritional vitamin B-12 deficiency in infants. Am.J.Dis.Child. 135:566-7.
- Heath, P.K. ed. 1983. Diet manual including a vegetarian meal plan. Loma Linda, LA. Seventh-day Adventist Dietetic Association.
- Hergenrather, J., Hlady, G., Wallace B. 1981. Pollutants in breast milk of vegetarian.
N.Engl.J.Med. 309:792.
- Ward, P.S., Drakeford, J.P., Milton J. 1982. Nutritional rickets in Rastafarian children.
Br.Med.J. 285:1242-3.
- Van Staveren, I.B., and Dagnelli, P. 1988. Food consumption, growth and development of Dutch children fed on alternative diets. Am.J.Clin.Nutr. 48:819-21.
- Truesdell, D.D. 1985. Feeding the vegan infant and child. J.Am.Diet.Assoc. 85:837-40.
- Robson, J.R.K. 1974. Zen macrobiotic problems in infancy. Pediatrics. 53:326-9.
- Sanders, T.A.B. 1988. Growth and development of British vegan children. Am.J.Clin.Nutr.
48:822-5.
- Vyhmeister, I.B., Register, U.D., Sommenberg, L.M. 1977. Safe vegetarian diets for children. Pediatr.Clin.North.Am. 24:203-10.
- Dunn Clinical Nutrition Centre. 1995. How much energy do you need? FEEDback
Newsletter for Nutrition Research Volunteers. (5) Spring 1995
- Newman, W.P., Freedman, D.S., Voors, A.W. et al. 1986. Relation of serum lipoprotein levels and systolic blood pressure to early atherosclerosis: the Bogalusa Heart Study. N.Engl.J.Med. 314:138-44.
- Dwyer, J.T. 1988. Health aspects of vegetarian diets. Am.J.Clin.Nutr. 48:712-28.
- WHO Report of a study group. 1990. Diet, nutrition, and the prevention of chronic diseases. WHO Technical Report Series 792.
- Kahn, R.H., Phillips, R.L., Snowdon, D.A., Choi, W. 1984. Association between reported diet and all cause mortality: twenty-one year follow up on 27 530 adult Seventh-day
Adventists. Am.J Epidemiol, 119: 775-87.
- Philips, R.L. 1980. Cancer among Seventh-day Adventists. J.Environ.Path Toxicol. 3:157-169.
- Schultz, T.D.. Leklem, J.E. 1983. Dietary status of Seventh-day Adventists. J.Am.Diet.Ass. 83:27-33.
- Berkel, J., De Waard, F., 1983. Mortality pattern and life expectancy of Seventh-day Adventists in the Netherlands. Int.J.Epidemiol. 12:455-459.
- Snowdon, D.A., Philips, R.L., and Fraser, G.E. 1984. Meat consumption and fatal ischemic heart disease. Preventive Medicine. 13:490-500.
- Fonnebo, V. 1985. The Tromso heart study: Coronorary risk factors in Seventh-day Adventists. Am.J Epedimol.122:789-793.
- Mills, P.K., Annegers, J.F., Philips, R.L. 1988. Animal product consumption and subsequent fatal breast cancer among Seventh-day Adventists. Am. J. Epidemol. 127:440-453. 37.Fraser, G.E., 1988. Determinants of ischemic heart disease in Seventh-day Adventists: a review. Am. J. Clin.Nutr. 48:833-836.
38. Pi-Snyder, X.F. 1991. Health implications of obesity. Am.J.Clin.Nutr. 53:1595S-1603S. 39 Prentice, A.M. 1995. Are all calories equal? In. Weight Controll. Ed. Richard Cottrell, Chapman & Hall, London.
- Kuczmarski, R.J., Flegel, K.M., Campbell, S.M., Johnson, C.L. 1994. Increasing prevalence of overweight among US adults: The Nationl Health and Nutrition Examination Surveys 1960 to 1991. J. Am. Med. Assoc. 272:205-211.
- Nutrition today newsbreaks. 1995. Shape-Up America programme launched. Nutrition Today. 30 (1) January/February 1995, p.5.
- Hill, J.O., and Prentice, A.M.1995. Sugars and body weight..Am.J.Clin.Nutr 62 (supplement), 178S-194S.
- Albanes, D. 1987. Caloric intake, body weight, and cancer: a review. Nutr.Cancer. 9:199-217.
- Lew, E.A. and Garfinkel, L. 1979. Variations in mortality by weight among 750 000 men and women. J.Chronic.Dis. 2:563-76.
- Hill, P., Chan, P.L., Cohen, L.A, Wyder, E.L., and Kuno K. 1977. Diet and endocrine related cancer. Cancer. 39:1820-6.
- Phillips, R.L., and Snowdon, D.A. 1983. Association of meat and coffee use with cancers of the large bowel, breast and prostate among Seventh-day Adventists: preliminary results Cancer.Res.[Suppl] 45:2403-8.
- Turjiman, N., Goodman, G.T. Jaeger, B., Nair, P.P. 1984. Diet, Nutrition intake and metabolisms in populations at high risk for colon cancer: metabolism of bile acids. Am.J.Clin.Nutr. 4:937-41.
- Ames, B.N. and Gold, L.S. 1990. Too many rodent carcinogens: Mitogenesis increases mutagenesis. Science. 249:970-971.
- Scrimshaw, N.S. 1996. Nutrition and Health from Womb to Tomb. Nutrition Today. 31 (2) March/April 1996.
- James, W.P.T., Ferro-Luzzi, A., Waterlow, J.C., 1988. Defenition of chronic energy deficiency in adults. Report of a working party of the International Dietary Energy Consultative Group. Euro.J.Clin.Nutr. 42:969-81.
- Olson, R.E. 1995. The folly of restricting fat in the diet of children. Nutrition Today 30 (6). November/December. pp. 234-244.
- Nutrition Today Newsbreaks. 1995. Fat in the diet of children. Nutrition Today 30 (3) May/June 1995. p100.
- Dunn Clinical Nutrition Centre. 1995. Obesity damages your health. FEEDback Newsletter for Nutrition Research Volunteers. (6) Autumn 1995
- Snowdon, D.A. and R.L. Phillips. 1985. Does a vegetarian diet reduce the occurrence of diabetes? Am. J. Public Health 75: 507-12.
- West, K.M. and Kalbfleish J.M. 1971. Influence of nutritional factors on prevalence of diabetes. Diabetes. 20:99-108.
- Gruchow, H.W., Sobocinski, K.A., Barbgoriak, J.J. 1985. Alcohol nutrient intake and hypertension in U.S. adults. J.A.M.A. 253: 1567-70.
- Sacks, F.M. and Kass E.H. 1988. Low blood pressure in vegetarians: effect of specific foods and nutrients. Am.J.Clin.Nutr. 18:795-800.
- Margetts, B.M., Beilin, L.J., Armstrong, B.K. 1988. Vegetarian diet in mild hypertension effects of fat and fiber. Am. J. Clin. Nutr. 48:801-5.
- Beilin, L.J., Rouse, I.L., Armstrong, B.K., Margetts, B.M, and R. Vandongen. 1988. Vegetarian diet and blood pressure levels: incidental or causal associated. Am.J.Clin.Nutr. 48:806-10.
- March, A.G., Sanchez, T.V., Michelsen, O., Chaffee, F.L., and Fagal, S.M. 1988. Vegetarian lifestyle and bone mineral density. Am.J.Clin.Nutr 48:837-41.
- Femel, M.B. 1988. Calcium utilization: effect of varying level and source of dietary protein. Am.J.Clin.Nutr. 48:880-3.
- Brand, T.S., Johnson, Q., Frank, F., Veith, W., Conradie, R., Hough, F.S. 1997. The influence of dietary crude protein intake on bone and mineral metabolism in sheep. (Submitted to Osteoporosis International).
- Johnson, Q., Veith, W., Conradie, R., Hough, S., Brand, T.S., Frank, F., Aalbers, J. 1997. Dietary crude protein and the occurrence of bone abnormalities in sheep. The effect of crude animal and plant protein source. (In prep).
- Johnson, Q., Veith, W.J., Brand, T., Frank, F. 1993. The effect of elevated dietary protein concentrations on calciuresis and its implications for osteochondrosis in sheep. XV International Congress on Nutrition, Adelaide, Australia.
- U.S. Department of Health and Human Services 1984. Osteoporosis consensus conference. Bethesda M.D. National Institutes of Health.
- Kjeldsen-Kragh, J., Haugen, M., Borchgrevink, C.F., Laerum, E. et.al. 1991. Controlled trial of fasting and one-year vegetarian diet in Rheumatoid arthritis. Lancet. 338:899-902.
- Phinney, S.D., Odin, R.S. Johnson, S.B., Holman, R.T. 1990. Reduced archidonate in serum phospholipids and cholesteryl esters associated with vegetarian diets in humans. Am.J.Clin.Nutr. 51:385-95.
- Carlson, E., Kipps, M., Lockie, A., Thomson, J.A., 1985. A comparative evaluation of vegan vegetarian and omnivore diets. J.Plant Foods. 6:89-100.