It is becoming more and more evident, that many degenerative diseases can be directly linked to dietary lifestyles. Moreover, the incidence of these diseases is also higher in Western cultures than in Eastern cultures. Western lifestyles are, however, becoming popular even in the East, and with this encroachment, degenerative diseases are becoming increasingly prevalent even in societies where these diseases were virtually unknown in the past. Besides coronary heart disease, the incidence of cancer in Western societies is very high, and most of the major cancers can be linked to lifestyles thus making them potentially preventable diseases. The most common cancers occurring in Western societies are listed in table 4.1.
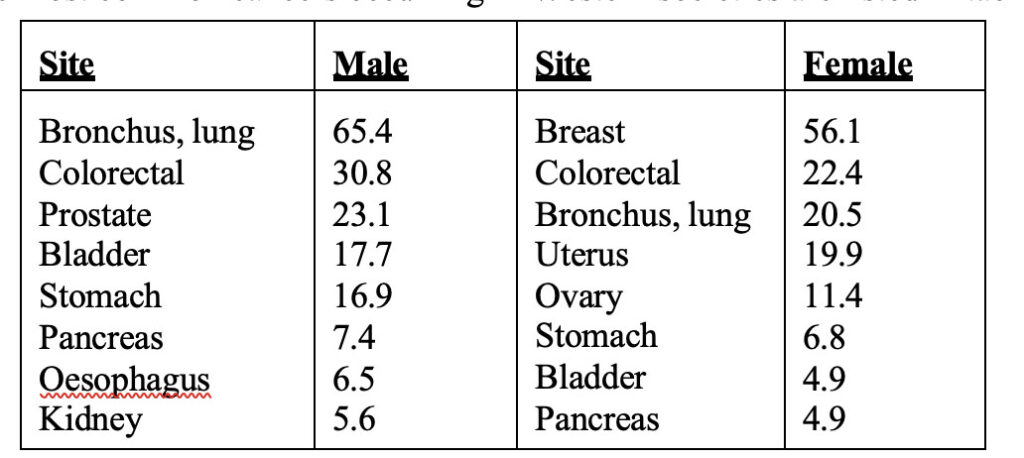
Table 4.1. Age standardized rates for the major cancers excluding skin in men and women in England and Wales. (From reference 1,2.)
In table 4.1 the major cancers are listed in order of prevalence, and the rates are age standardized. However, the risk of cancer increases with age, and the age specific incidence of cancer can give a clearer picture of the risk for various age categories. These figures are presented in figure 4.1.
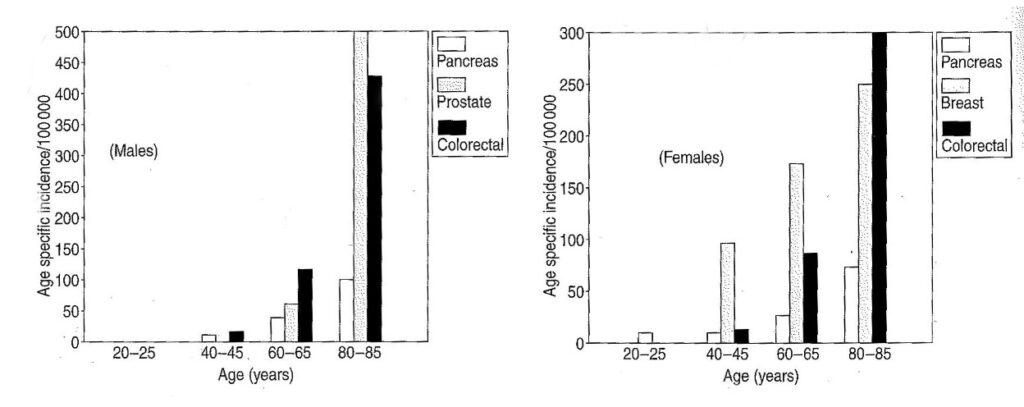
Figure 4.1. Age specific incidence rates for various cancers in males and females in England and Wales. (Adapted from references 2,3)
Even when age is taken into account, major discrepancies between the incidence of the various cancers occur in different countries, indicating that national lifestyle choices impact directly on the prevalence of cancer in these societies. These differences are not as a consequence of inheritable differences in resistance to cancer among the different races and nationalities, but are directly related to lifestyle choices. A well studied example of this impact, is the change in incidence of colorectal cancer in Japan with the adoption of a more Western orientated lifestyle. Whereas the rates for colorectal cancer were once low in Japan, there has been a rapid increase in age specific incidence of this cancer since 1960, and rates are approaching those recorded in Britain (Figure 4.2.)
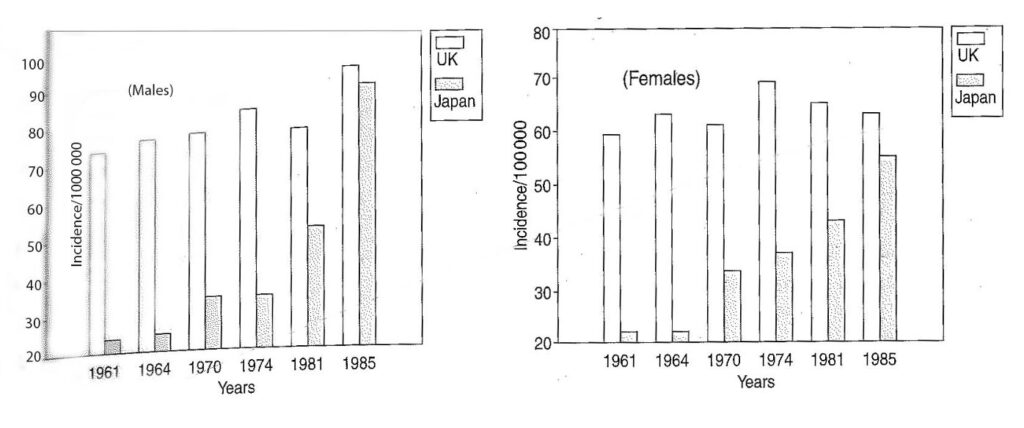
Figure 4.2. Age specific colorectal cancer incidence rates in men and women aged 55-60 in Japan and the UK. (Adapted from references 1,2,3)
As discussed in the previous chapters, a healthy diet is one that relies on a high complex-carbohydrate intake whilst at the same time limiting the consumption of proteins and fats. Diets rich in animal products, on the other hand, are high-fat, high-cholesterol, high-protein diets and carbohydrates, including fibre, are present in negligible amounts. By definition therefore, diets high in animal products must therefore be considered a health risk. In spite of these facts, the media encourages humanity to consume more and more animal products to prop up and maintain the vast economic empires that have been erected upon the foundations of the animal-products industry. Consumers are brought under the wrong impression by the advertising claims of manufacturers, and as a result there has been a dramatic rise in the consumption of animal products in the industrialized world over the past few decades. Moreover, some of the advertising claims have even left their mark on the medical profession, which often prescribes diets rich in animal products such as dairy products to ensure adequate supplies of essential nutrients.
Consumption of animal products has risen sharply in the United States since the US Department of Agriculture began keeping records in 1910, whereas consumption of fruits, vegetables and grains has declined drastically. Meat, fish and poultry only contributed 30% of the total protein consumption of Americans from 1909-1933, but this figure gradually rose, together with that of dairy products, so that these commodities today supply a staggering 70% of proteins consumed by that nation, and a similar trend is apparent in other industrialized nations.
The consumption of animal products has been positively associated with mortality because of disease, particularly heart disease, diabetes and cancer. In a study on the cause of mortality, carried out on vegetarians and non-vegetarians in California, it was found that the consumption of animal products could be correlated with mortality from degenerative diseases. It was found that meat consumption could be positively correlated with all causes-combined-mortality in males whereas there was a positive correlation of egg consumption and all causes-combined-mortality in females.4 Meat consumption particularly increased the relative risk of mortality from coronary heart disease, diabetes, colon cancer and prostate cancer in males (fig 4.3a), whereas in females, meat consumption could be positively correlated with mortality from coronary heart disease, and ovarian cancer (fig 4.3b).
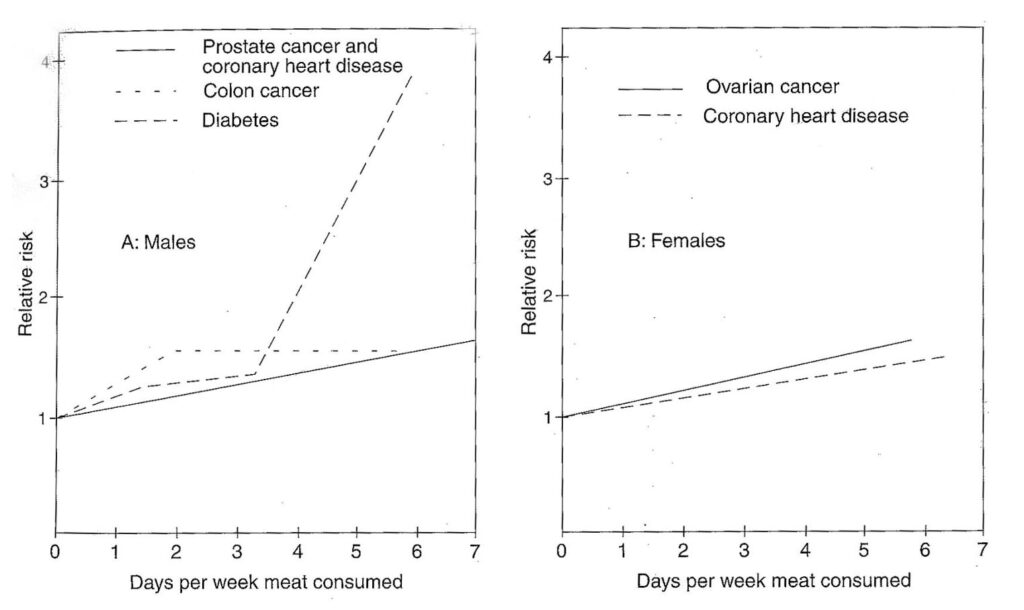
Figure 4.3. Meat consumption and age-adjusted relative risk of mortality in men (a) and women (b). The relative risk is calculated by dividing the mortality rate of meat eaters by the mortality rate of non meat eaters. A relative risk that is >1.00 (greater than one) suggests that the exposed group has a greater likelihood of dying from the disease in question than the non-exposed group. (Adapted from reference 4 and 5)
Meat is not the only animal product that increases the risk of mortality. Dairy products and eggs show similar trends. In the case of eggs, there was a moderate increased risk in males from diseases such as colon cancer and prostate cancer (fig 4.4a), and in females there was a moderate to high risk of mortality from colon and ovarian cancer (fig 4.4b).
The consumption of dairy products could also be correlated with increased incidence of disease-related deaths, particularly as a result of prostate and colon cancer in males, and in females there was a moderate correlation with breast cancer. Milk consumption, in particular, was linked to an increased risk of prostate cancer (fig 4.5).
It is true that opposite effects are also obtained, and that relative risk is in some cases reduced when animal products are consumed, but the bulk of the evidence strongly links their consumption to increased mortality rates from disease-related causes. The reasons for these statistics are however numerous, and vary from product to product.
MEAT
Diets high in meat are usually low in carbohydrates, particularly fibre. The levels of proteins are very high, and these high protein levels can cause numerous problems. Not all the protein ingested is completely digested, and approximately 2g of nitrogen in the form of undigested protein, peptides and amino acids (equivalent to 12g of protein) enter the large bowel daily. The bacteria in the large bowel will preferentially utilize carbohydrate residues to meet their energy needs, but when carbohydrate levels are low and protein levels high, then amino acids will be metabolised resulting in the release of ammonia and phenol, both of which are potentially harmful. Cooked and smoked meat products, in addition, also contain other potentially harmful substances such as polycyclic aromatic hydrocarbons, heterocyclic amines, and N-nitroso compounds, which have been linked to degenerative diseases.
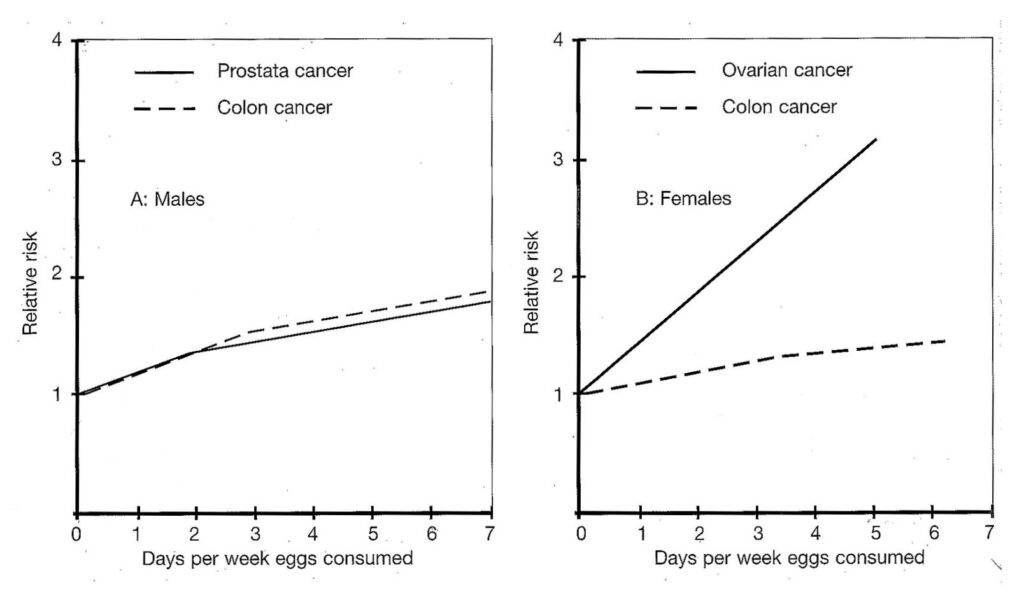
Figure 4.4 Egg consumption and age-adjusted relative risk of mortality. (Adapted from references 4 and 5)
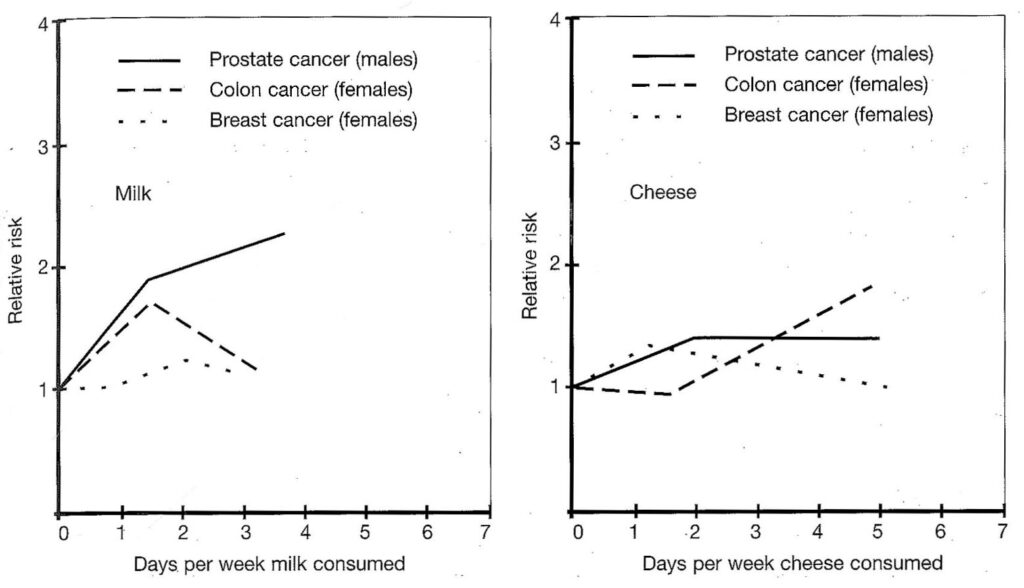
Figure 4.5. Dairy product consumption and age- adjusted relative risk of mortality. (Adapted from references 4 and 5)
These potentially harmful substances should be eliminated from the system as rapidly as possible, and if sufficient fibre were present in the diet, then the time that food is retained in the intestines would be considerably reduced. In the case of a relatively high intake of cereal fibre, the partly fermented residual polysaccharides, derived from these fibres, would absorb water, and this would lead to increased faecal mass and decreased transit time, thus reducing the time that potentially harmful substances such as carcinogens remain in large bowel.4,6 With a high meat consumption, however, the harmful substances can remain in the intestines for much longer periods, and this exposure has been linked to increased cancer rates. In this regard, the relationship between colorectal cancer and meat consumption is well established and is presented in figure 4.6.
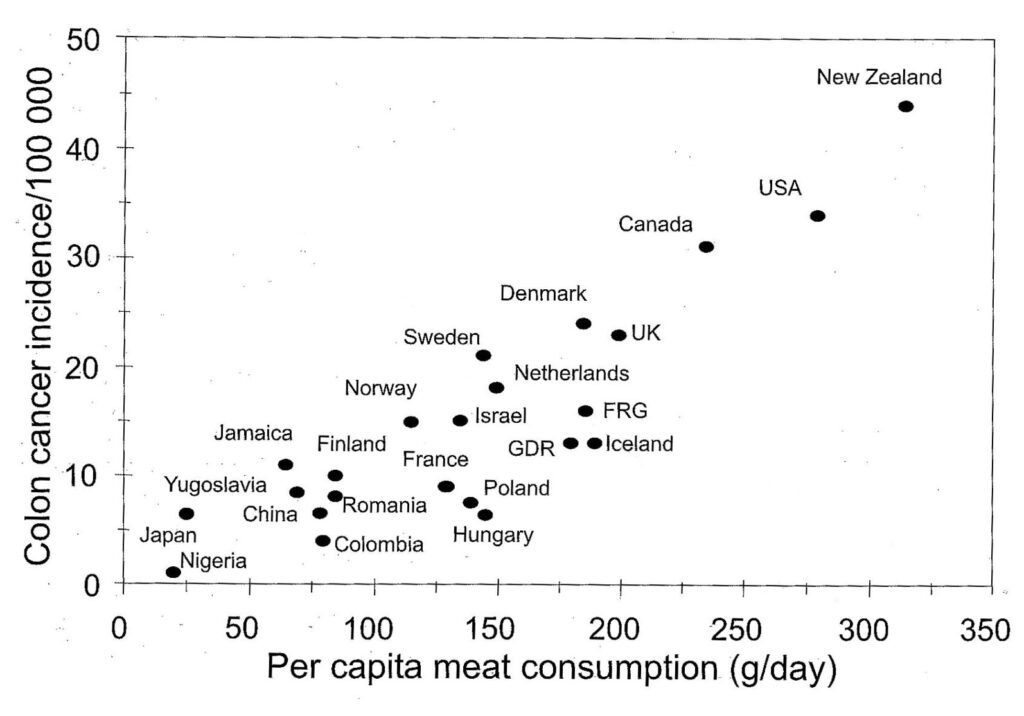
Figure 4.6. The relationship between meat consumption and colorectal cancer in various countries. (Adapted from references 2,7).
Colorectal cancer is the second most prevalent cancer in Western societies and affects up to 6% of men and women by the age of 75. Different factors seem to be responsible for colorectal cancer in the various countries, because the cancers manifest themselves differently, probably due to different induction modes. In high risk countries, the majority of colorectal cancers are located in the lower bowel, near the rectosigmoidal junction, whereas in low risk countries the majority of cancers are situated in the right side of the colon. Besides being low in fibre, the compounds in meat most commonly linked to the promotion of tumours are ammonia, phenols, polycyclic aromatic hydrocarbons, heterocyclic amines, and N-nitroso compounds.
Ammonia
Within the gut, the limited availability of carbohydrates in high-meat diets will lead to an increase in ammonia concentration in the colon because bacteria will metabolize the protein residues which enter the gut when carbohydrate levels are low. Ammonia, in turn, increases cell proliferation and alters DNA synthesis and has, therefore, been implicated in colon cancer.4 It is known that increased cell proliferation is associated with cancer in humans.8 Ammonia will not only be liberated from animal proteins, but from excessive intake of plant proteins as well. A high plant-protein intake is, however, usually associated with a high fibre intake and this would shorten the exposure time. This is particularly true in the case of whole foods with their high concentrations of fibre. High ammonia levels are not only a problem within the gut, but also effect the whole organism. As discussed in the chapter on proteins, the consumption of high levels of proteins will necessitate the deamination of amino acids in order to meet the body’s energy demands. This will require efficient detoxification of the produced ammonia, which in mammals is achieved via the urea cycle. As the amino acid arginine plays a principle role in this cycle, the higher levels of this amino acid in plant proteins than in animal proteins offers a possible protection against ammonia toxicity.
Phenols
A high-meat, low-carbohydrate diet will also allow more aromatic amino acids, such as phenylalanine and tyrosine to enter the colon. Gut bacteria produce cresol and phenol when they metabolize these amino acids. Both cresol and phenol have been associated with the promotion of skin and colon cancer9 and rapid elimination of these compounds seems advisable, even if their effect on the gut mucosa has not been fully resolved. A diet rich in fibre can once again assist in clearance of these compounds by decreasing the food transit time. Amino acid metabolism will also increase the concentration of these compounds in the blood, and elimination of these compounds is normally done by the kidneys. Nevertheless, consistently high levels of these compounds can be associated with diets rich in animal products, as it is known that urinary phenol levels increase when subjects are fed high-meat diets and to decrease with an increase in dietary fibre.10 Low phenol levels could thus limit the risk of cancer, and a whole-food diet is ideal to achieve both low levels of these compounds and high levels of fibre.
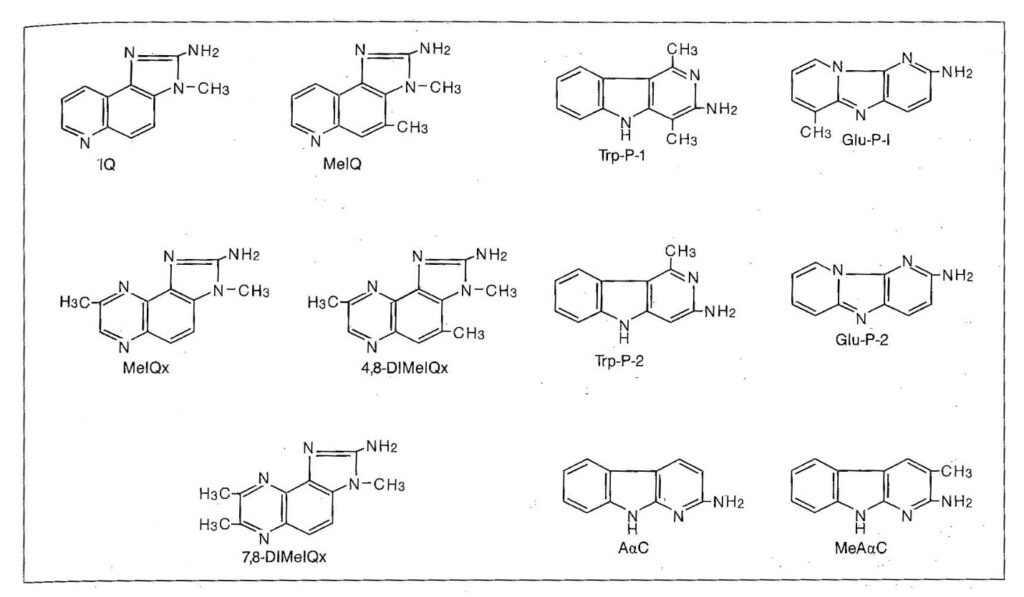
Figure 4.7. The chemical structure of heterocyclic amines. (Adapted from reference 14)
Polycyclic aromatic hydrocarbons (PAH)
Polycyclic aromatic hydrocarbons (PAH) result primarily from atmospheric deposition onto plants in smoky areas. One such hydrocarbon is Benzo(a)pyrene, a potent carcinogen, which is also formed in foodstuffs that are smoke-dried (such as tea) and also during the smoking and grilling of animal foods. PAH also occur in shell-fish that come from a polluted marine environment.11 Fats are once again a prime source of PAH and smoked and grilled food in particular are subject to contamination by these carcinogens.12 Avoidance of high risk foods seems desirable if the risk from these compounds is to be curtailed.
Heterocyclic amines
Heterocyclic amines are mutagenic and carcinogenic compounds that are formed in cooked and charred foods.12 They form particularly in meat and fish even if cooked at relatively low temperatures.13 In fact, it is estimated that the average consumption of these compounds is as high as 100µg per person per day,14 but other calculations place daily consumption in the range of 0.4 to 16 µg/day.2 Heterocyclic amines have been found to elicit carcinogenicity in the liver, lung, oral cavity, stomach and intestines of rats and mice, and have also been implicated in cancer of the lymphatic systems, blood vessels, skin and mammary glands. Over 20 mutagenic heterocyclic amines have been isolated from cooked animal products, and well done portions of meat contain higher concentrations than medium or rare portions. To obtain these compounds for experimental purposes, a standard protocol of grilling or frying for 6 min. at 200°C is used. Generally, frying, grilling and barbequing produce more of these compounds than does stewing, steaming, microwaving or poaching.2
The chemical structures of these compounds and the concentrations found in some foods are presented in figure 4.7 and table 4.2.
Heterocyclic amines are relevant carcinogens in humans, but in the case of colon cancer their relative contribution may be small (0.25% of all colon cancers).2 Food that will be particularly suspect in terms of heterocyclic amines will be cured and baked or fried meats. Even beer, soybeans, protein isolates and fried mushrooms were found to contribute significantly to the daily intake of these compounds. A study of heterocyclic amine formation in swine meat heated to 200°C showed that the main reactants of the mutagen-forming reactions are amino acids and creatine.15
N-Nitroso compounds
These compounds have been linked to human cancer of the oesophagus, stomach, bladder and possibly lung.16 Beer as well as nitrite-cured meat products, especially bacon after frying, and salt-dried or smoked fish, are major sources of these compounds. Incidentally, the mainstream smoke from one cigarette contains up to 65µg volatile nitroso amines and the side stream contains up to 1000µg,13 a healthy lifestyle thus constitutes more than just eating correctly. It is difficult to estimate what the level of exposure to these compounds is, particularly since it is known that nitroso amines are efficiently metabolized in the liver. Nevertheless, these compounds have induced liver and oesophagus cancer in experimental animals.12,13 Intestinal bacteria can also catalyse the formation of nitroso amines and this has been linked to gastric cancer. Nitrosated amides are direct acting carcinogens, and cause tumours near to the site they are produced, whereas nitrosated amines require hydroxylation and can initiate tumours at distal sites.2 In one study, increased consumption of red meat caused a 3-fold increase (from 40 to 113µ g/day) in N-Nitroso compounds in the faeces of eight volunteer males who were subjected to low and high meat diets, but white meats did not seem to induce similar effects. The increase is high, when one considers that smoking 40 cigarettes a day produces an exposure to approximately 30µ g/day of tobacco-specific carcinogenic N-Nitroso compounds.17
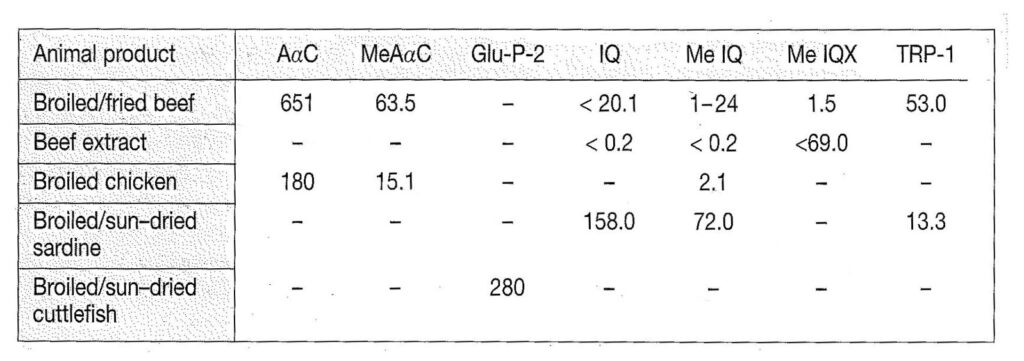
Table 4.2. The occurrence of heterocyclic amines in animal products. Concentrations are in µg/kg. (Adapted from reference 14)
Biological magnification
In addition to the aforementioned compounds, animals are also known to concentrate environmental pollutants such as heavy metals, pesticides, herbicides and industrial toxins. These toxins become concentrated in the tissues of organisms as they pass through the food chain. The concentrating process is called biological magnification and is responsible for widespread decimation of animal life on earth. Moreover, if species are harvested for human consumption from the top of the food chain (largely marine species), then these concentrated toxins are transferred to the human consumer. The extent of biological magnification of toxins such as DDT is well documented, and it has been shown that the concentrating potential can induce several million fold increases in the concentration of these substances in the tissues of animals. Concentrations of DDT in the water as low as 0.000005 parts per million can be concentrated to over 26 parts per million in top carnivores.
Animals accumulate toxins particularly in their fatty tissues, and when called upon to utilize their fat reserves, the release of these toxins into the bloodstream can lead to various diseases and death. In this regard, it has been established that the deaths of hundreds of thousands of marine mammals can largely be attributed to lowered immune capacity owing to the immune system being compromised by the presence of accumulated toxins. It has been found that even the paint used on the hulls of ships can add sufficient toxins to the oceans to cause widespread death of marine life. The paint contains tributyl tin (TBT) which prevents barnacles from sticking to the hull of vessels. The substance has been banned for use on small vessels but is still widely used on larger vessels. TBT is probably the most potent toxin deliberately introduced into the sea, as even a few nanograms in water can cause abnormal development such as female dog whelks developing male organs. However, the immunosuppression capabilities of the toxin could be one of the factors contributing to the widespread death of dolphins and other marine life. It was found, that marine mammals concentrate TBT in their tissues in concentrations of up to 10 parts per million.18
Marine pollution is a worldwide problem, particularly in industrialized or highly populated areas. In the Mediterranean, more than 500 million tonnes of sewage alone pours into the water every year. Sewage is not the only pollutant flowing into this sea, it is estimated that annually 120 000 tonnes of marine oils, 60 000 tonnes of detergents, 100 tonnes of mercury, 3 800 tonnes of lead, 1 million tonnes of crude oil and 3600 tonnes of phosphates enter this sea. In 1985 the Mediterranean nations set themselves cleanup goals which were to be achieved by 1995, but none of these goals have been achieved.19 If the wealthier nations of the world are struggling with clean up goals, one wonders how the less fortunate are faring.
It is known that fish and shell-fish in particular, concentrate heavy metals such as mercury in their tissues, and these compounds can also be carcinogens. Already in 1953, cats and birds on the island of Minamata in Japan got the ‘staggers’ and died. Then the humans developed headaches, ataxia, fatigue, foetal deformities and mental abnormalities. Some 15 000 people were affected and at least 3500 died. A government investigation showed that the culprit was mercury salts that had been dumped in the river and had accumulated in the sediment of Minimata Bay. There the salts had become methylated and converted to methyl mercury, a highly toxic organic compound. Once this compound had found its way into the food chain, it was accumulated in the tissues of marine organisms, and biological accumulation led to high concentrations in tuna which in turn was consumed by the human population. A more recent episode involving mercury pollution can be found in the pollution of the river Rhine in Germany in November 1986, when a blaze in the giant chemical company Sandoz caused some 30 tonnes of mercury and pesticides to be washed into the Rhine. Only direct and targeted intervention by the industrialized European nations prevented this disaster from permanently destroying the delicate ecosystem of this river.
The TBT example illustrates the fact, that very minor concentrations of toxins can attain catastrophic proportions due to biological accumulation, not to mention the very high levels of pollutants in some areas. Humans that rely largely on animal products for their sustenance, will experience similar accumulations of toxic compounds as do the top carnivores in nature, and a reduction, or even avoidance of animal products can thus enhance the capacity to cope with disease.
DAIRY PRODUCTS
Milk and dairy products are advertised as wonder foods that will supply all the nutrients required for healthy growth. The calcium levels in milk, in particular, are stressed as an essential component of the human diet, and the impression is created that a loss of this dietary source of calcium will lead to abnormal bone development. It is certainly true that dairy products are packed with nutrients, but this does not mean that the combination of nutrients is suited to human nutrition. Mother’s milk is essential for infants, but then infants are specially designed to cope with this growth-promoting food. Prior to weaning the necessary enzyme systems needed for the digestion and assimilation of milk components are active, but they are progressively deactivated with age. The milk of other mammalian species also differs in composition from mothers milk, and this, together with the potential danger from ingested antigens, makes cows milk unsuitable for human consumption.
There is considerable resistance from industry, and even from the established scientific world, to the idea that dairy consumption is detrimental to health, but the evidence from recent scientific findings seems fairly conclusive with regard to this issue. Dairy consumption is being coupled with a host of diseases, and as consumption rises world-wide, so the evidence is becoming more and more conclusive. In the past, the detrimental effect of the consumption of dairy products may have been masked by the positive effects of other lifestyle choices such as higher consumption of grains, fresh fruits and vegetables with their high fibre content. Western diets have, however experienced a sharp increase in the consumption of animal products, including dairy products, with concomitant decline in the consumption of grains, legumes, fruits and vegetables, and this may explain the increase in the incidence of degenerative diseases in industrialized countries.
Lactose intolerance
Lactose, the sugar in milk, is broken down in the intestines by the enzyme lactase. Most people are able to digest lactose properly during infancy and early childhood, but as they grow older this ability declines. Approximately 75% of adults worldwide are lactose intolerant and those with the highest intolerance are Native Americans and Asians and only slightly lower than these are the blacks, Jews, Hispanics, and southern Europeans. Lactose intolerance is lowest among northern Europeans and their descendants. In the US some 25% of Caucasians, 51% of Hispanics and 75% of all African Americans, Jews, and Native Americans have insufficient levels of lactase to digest dairy products and 90% of Asian Americans are lactose intolerant.20,21 It has been found that 90% of African people are lactase deficient, and in the case of the rural Zulu of South Africa it was found that they showed no change in blood glucose concentrations after ingesting 50g of lactose.22 When milk and dairy products are digested, lactose is broken down by the enzyme lactase into glucose and galactose (fig. 4.8).
The presence of lactose is a feature of mammalian milk, but the concentration of this sugar is normally geared to the needs of the species, as are the concentrations of all the other components of milk. In the case of humans, mother’s milk does not only contain the essential nutrients that are required for growth and development, but also contains the bacterium bacillus bifidus that assists in the digestion of lactose. In cow’s milk, however, the bacterial composition differs from that of human milk, and if cow’s milk is fed to infants, this can interfere with the digestion of lactose. Moreover, human milk has a higher carbohydrate concentration (7%-7,5%) than cow’s milk (4,5%-5%) and contains some 200m mol/litre of lactose which makes it sweeter than cow’s milk. The lower protein and higher carbohydrate content of human milk is also more suited to the needs of infants, because their growth rates are considerably lower than those of calves.
After the conversion of lactose to glucose and galactose, the available galactose is not utilized as such, but is converted to glucose in the liver by a series of steps requiring the initial presence of the enzyme galactokinase. The production of both the enzymes lactase and galactokinase declines with age, and the capacity to digest and utilize the products of lactose in adult life is thus curtailed. A deficiency in the enzyme lactase will result in fermentation of lactose by intestinal bacteria, which can result in abdominal distress such as the development of excessive gas, cramping, bloating, borborygmi (stomach rumbling), altered bowel habits and diarrhoea.21 The severity of the symptoms depends on the quantity of lactose consumed and the level of intolerance.
Milk protein intolerance
A further problem with milk is encountered in the digestion of the milk protein casein. In comparison to human milk, cow’s milk contains 300% more casein and more than double the amount of total protein. Casein and β-lactoglobulin are the two main proteins in milk and they are unique in that they contain a perfect blend of amino acids, which is precisely what is needed during early infant growth. Human infants, however, double their mass on average 180 days after birth, whereas cows achieve the same feat in only 47 days. Cow’s milk is therefore geared to meet the rapid growth requirements of cows, but is not suitable for humans. Casein also naturally stimulates normal thyroid function in infants, and as the thyroid is involved in many developmental processes, including the development of the nervous system, casein from other mammalian species could have adverse effects on metabolic processes of infants particularly since a portion of the dietary casein can be absorbed undigested and serve as antigen.
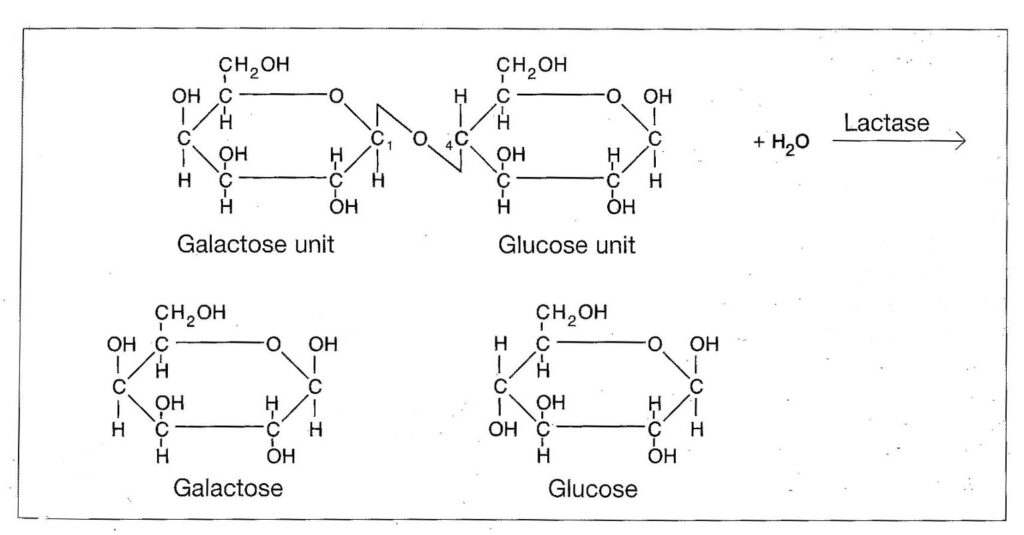
Figure 4.8. The digestion of lactose.
As is the case with the enzyme lactase that digests lactose, the concentration of the enzyme rennin, that breaks down the casein, also declines with age in all mammals, and by the time milk teeth develop it is virtually non-existent in the human digestive tract. Without rennin, the digestion of casein has to be carried out by the normal proteolytic enzymes which are not as efficient in breaking down casein. The presence of casein in the diet of mammals has also been linked to elevated cholesterol levels and various degenerative diseases such as arteriosclerosis. Rabbits fed casein developed arteriosclerosis, but the effect could be reduced if a plant protein source, such as soybean flour was introduced into the diet. This shows, that the amino acid pool produced by casein probably no longer meets the requirements of weaned or adult mammals. Casein also produced higher cholesterol levels than soy protein in a number of animal species, including rats, hamsters, guinea pigs, pigs, and monkeys. In humans, a reduction in cholesterol levels was also found if meat and dairy proteins were replaced by soy proteins.23,24 Casein also seems to have an adverse effect on insulin secretion, thyroxine levels, gastrointestinal hormones and it has an adverse effect on calcium metabolism.
Calcium in dairy products
A matter which has received much media attention, is the calcium content of milk and dairy products. It certainly is true that dairy products do contain fair amounts of calcium, but a large proportion of the calcium in milk is combined with casein in the form of calcium caseinate. Dairy products are also not the only source of calcium available to humans, as grains, legumes, seeds, nuts and many vegetables are excellent sources of calcium. Moreover, fractional absorption of calcium from these sources is higher than from milk. A study done on whole-wheat products showed that fractional calcium absorption from whole-wheat bread exceeded the absorption of calcium from milk, ingested at a comparable load, in the same subjects.25 Not only is the absorption rate of calcium higher from plant sources, but animal sources seem to cause calcium loss in view of the nature and the concentration of the proteins which they contain. Table 4.3 lists the calcium levels in some dairy products and plant foods.
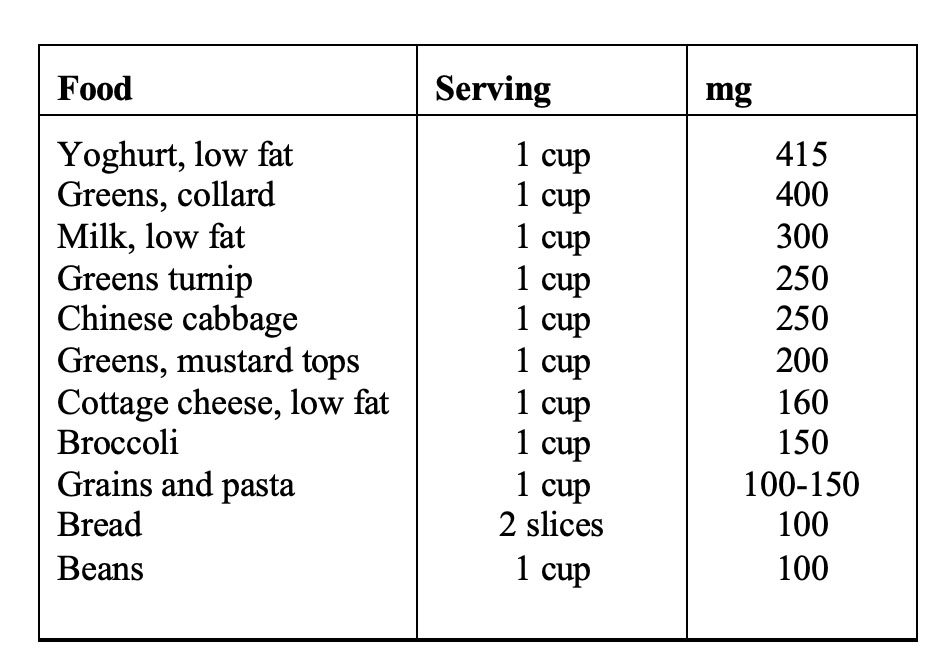
Table 4.3. Calcium levels in selected foods. (From reference 26)
Foods vary in their composition, and in the case of seeds, grains, beans and vegetables, there are considerable differences in calcium content of different varieties and in general, dark green vegetables are a good source of calcium. In addition to the foods listed above, almonds, sesame seeds, sunflower seeds, soybean products such as bean curd and soy flower, carob, chick peas, haricot beans, mung beans, garlic, parsley, watercress and dried fruits (especially figs) are good sources of calcium.
Calcium utilization is governed by complex processes, and the absorption, bone deposition and excretion of calcium is strongly influenced by other dietary components. It is well documented that increased protein consumption causes calcium loss in the urine,27,28 and this is particularly true in the case of proteins from animal products.29 An investigation into the effects of various protein diets on calcium retention showed that proteins from dairy products, such as cottage cheese, caused considerable calcium loss in the urine.30 The culprit here seems to be casein, and other studies seem to corroborate this. In one study it was found that casein fed to weanling rats caused kidney calcification, an effect which was not observed if the protein came from another source.31 If calcium losses exceed absorption, then a negative calcium balance exists, and calcium must be mobilized from bone in order to maintain plasma calcium levels in a dynamic state. This loss of calcium from bone can eventually lead to osteoporosis. It is, therefore, not surprising that osteoporosis seems more prevalent in countries where the consumption of dairy products is high.32,26 In table 4.4 the incidence of osteoporosis in various countries in relation to the consumption of proteins and dairy products is presented, and in figure 4.9, the relationship between dairy consumption and osteoporosis (expressed as hip fracture rate per 100 000 women) is presented.
Although dairy products are rich in calcium, paradoxically, it is apparent from the above data that the calcium from milk is not synonymous with healthy bone structure (see chapter 5 for more information on dairy free diets and osteoporosis). Moreover, calcium supplementation does not provide a solution for the dilemma, as countries, such as the United States, with the highest supplementation rates still have among the highest rates of osteoporosis. Not even in lactating women does calcium supplementation seem to have much of an effect in either white or black women. In one study on White, middle class women it was found that absorption of calcium from the intestines was not increased during supplementation compared to lactating women on low calcium diets. The calcium needs for milk production were met by decreased urinary excretion and increased bone resorption and not by increased intestinal absorption despite high calcium intakes.33
In a study on Gambian women similar results were obtained. Gambian women normally have a low calcium diet based largely on rice, millet, groundnuts and fish. This diet provides less than 300 mg/day of calcium which is considerably lower than current recommendations for lactating women. Increasing the calcium level threefold to bring it line with FAO/WHO recommendations had no discernable effect on breast milk calcium concentrations or on the maternal bone mineral content. This suggests that there was no benefit from increasing the calcium intake during lactation.34 The women in the supplementation group had consumed a total of 0.26 kg (one quarter to one third of the whole- body calcium content) after 52 weeks, and showed significantly greater urinary calcium output (7% of the dose). As the bone mineral content did not change, the researchers concluded that the rest of the additional calcium was just not absorbed from the intestinal tract.34 This study underlines the fact that calcium needs can be adequately met by even low calcium diets that contain no dairy products.
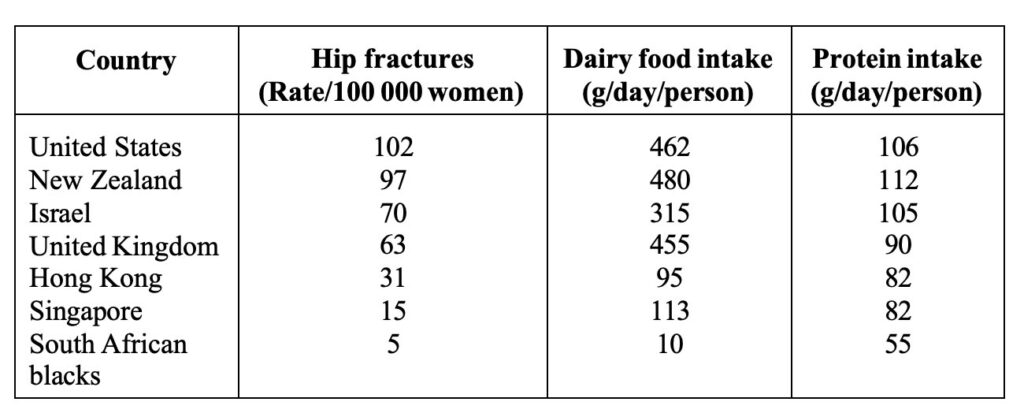
Table 4.4. Correlation between osteoporosis, dairy food and protein consumption by countries. (Adapted from reference 26).
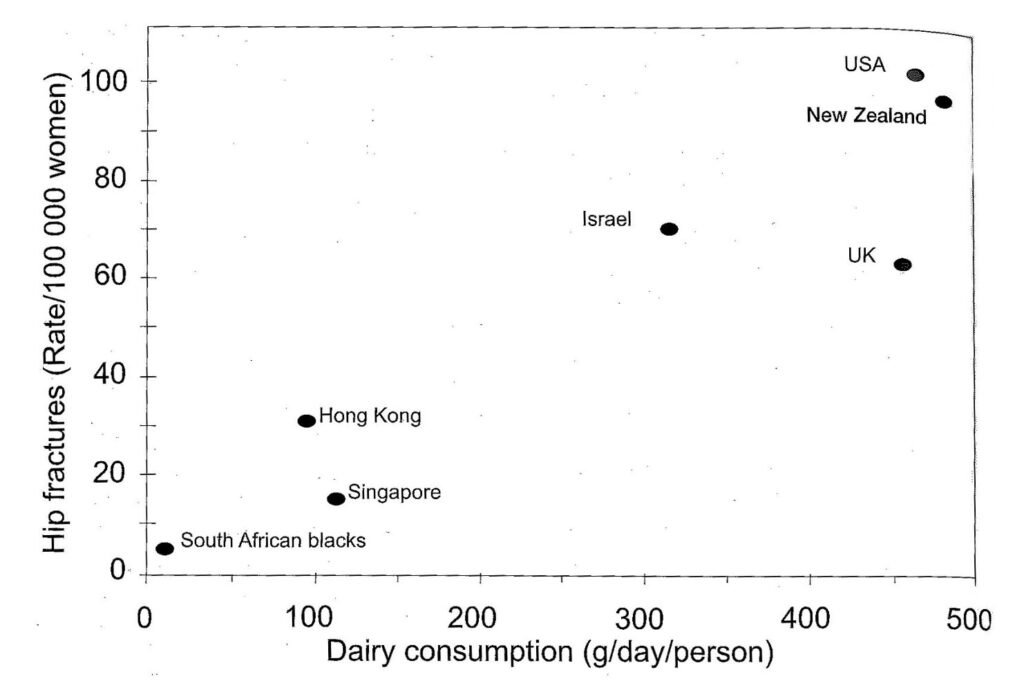
Figure 4.9 Correlation between osteoporosis and dairy food consumption by countries. (Adapted from reference 26).
In our own laboratory we have consistently found that animals (sheep, rats, rabbits and vervet monkeys) fed animal proteins, particularly casein or dairy products showed significant increases in urinary calcium levels, compromised bone status, and in common with the other studies, reduced intestinal absorption. In a current study on Vervet monkeys conducted at the Primate Unit of the Medical Research Council in South Africa two groups of monkeys were fed diets containing equivalent quantities of calcium, but one group received largely milk powder as protein source whilst the other group received kidney beans and maize as protein source. Stool calcium analyses showed that absorption of calcium was significantly lower in the dairy group than in the bean/maize group irrespective of whether they were on a high (17%) or low (8%) protein diet thus demonstrating the adverse effect of dairy products on calcium utilization.35
Dairy products and the immune system
Human milk not only contains less protein than cow’s milk, but the distribution of proteins is also different. A group of proteins that are particularly important in this regard are the immune globulins which carry antibodies and are particularly numerous in the early milk known as colostrum. These globulins contain antibodies found in the mother’s blood and transmit immunity to the newborn infant. When mother’s milk or cow’s milk is ingested, the system is capable of transporting these antibodies directly into the blood-stream via carrier systems, an ability that persists to a lesser extent even in adults. Human milk contains antibodies which differ from those found in cow’s milk and when cow’s milk is substituted for mother’s milk, the immunoglobulins from the cow’s milk will interact with the immune system and this can lead to an allergic reaction. Many allergies can primarily be attributed to milk, and will disappear when milk is removed from the diet.
Allergic disorders are a widespread health problem of particularly infants and young children in the developed world, and according to several population studies, the incidence and severity of these disorders has increased significantly of late.36 Cow’s milk is a major source of allergies and has been implicated in virtually all the common ailments of the respiratory tract. Hay fever, sinusitis, chronic bronchitis, colds, ear infections and even asthma can largely be ascribed to the intake of dairy products.37,38,39 In addition to these ailments, children are prone to diarrhoea, vomiting, constipation, colic, growth retardation, psychological disturbances, eczema and asthma if fed cow’s milk. Allergies need not immediately be apparent and can manifest later in life. Moreover, once an allergic reaction to a substance is manifested, greater sensitivity to other antigens is induced.37 A causative factor in congestive diseases is the ability of dairy products to promote mucus formation, and milk, cheese, butter and cream are the most likely of all foods to promote the build up of mucus.
Cow’s milk also causes colic in infants. The relationship between cow’s milk and colic is well established, and in infants that are breast fed, but also receive cow’s milk, colic is very common. Once cow’s milk is removed from the diet, however, colic disappears in most cases.40 Cow’s milk allergy is frequently the first manifestation of allergy because the proteins in cow’s milk are the first foreign antigens encountered in large quantities in infancy.36 Allergy to cow’s milk is most prevalent at the age of 1 year and has been reported in 2.8% of the general child population, but in infants with atopic dermatitis the incidence of cow’s milk allergy is at least five times that figure.36 Atopic dermatitis is a chronic eczematous skin disease which frequently begins in infancy and probably results from the repeated ingestion of allergins. This in turn leads to frequent scratching and the consequent
trauma induced lichenified lesions. It has been established that casein from cow’s milk causes an increase T-cell frequency and a specific T-cell-mediate immune response to casein can be found in the blood of adolescent and adult patients who suffer from milk-related exacerbation of atopic dermatitis.40
Cow’s milk has been linked to the development of insulin-dependent diabetes (IDD). IDD results from a chronic autoimmune process that can exist for years in a preclinical phase, with the classic manifestations of the disease (hyperglycaemia and ketosis) only occurring after most of the insulin-producing beta cells have been destroyed. There is evidence, that T lymphocytes are a major contributor to the pathogenic process. In this regard, cow’s milk has received much attention because people who were not breastfed or breastfed for only a short period of time are at increased risk of IDD. It is noteworthy, that 100% of newly diagnosed patients with IDD have antibodies to bovine serum albumin. Moreover, the pancreatic beta- cell proteins display substantial molecular cross-reactivity with bovine serum albumin from cow’s milk. IDD can thus be an abnormal response to the foreign protein leading to an immune response to both bovine serum albumin and the pancreatic beta-cell protein. 41
The findings by Cavallo et al 42 of peripheral blood T-cell reactivity to β-casein in half their 47 patients with IDD adds weight to the cow’s milk hypothesis.43 There have been arguments for and against the cow’s milk hypothesis, since IDD also occurs in infants that have never received cow’s milk. However, it has now been conclusively shown that the antigens in cow’s milk are transferred to the mothers milk if she consumes cow’s milk. In a study done on Japanese women it was found that β-Lactoglobulin was transferred to the mother’s milk because it is resistant to acid and enzymatic degradation and if taken orally is absorbed into the system.44 Moreover, there have been reports of infants that are only breastfed and never received milk protein developing allergies to cow’s milk, which was then alleviated when the mothers eliminated dairy products from their diets.44
Finally, the consumption of dairy products has been implicated in intestinal ulcers45 and cancer. Milk consumption in particular has been positively correlated with prostate cancer,5 and in an Italian case study, risk of breast cancer was positively associated with the intake of milk and dairy products.46 For infants, the best food is mothers milk and cow’s milk should be avoided at all costs. Mothers milk will ensure the normal development of infants at every level. It has even been established that the intelligence quotients (IQ) of children that were fed breastmilk are significantly higher than those of children that did not receive breastmilk even after adjustment for differences between groups, mother’s education and social class. 47 For those that have become accustomed to the consumption of milk, the replacement of dairy products with legume, seed or nut milks and creams will provide a more than adequate alternative to milk.
Dairy products and infertility
The issue of a rise in infertility, particularly male infertility, has produced considerable controversy in scientific circles. More and more reviews have appeared in the scientific literature claiming a decline in semen quality which is being largely attributed to environmental factors such as exposure to oestrogens (dietary, pharmaceutical and environmental pollutants). It has been suggested that environmental factors, possibly acting in fetal and early neonatal life, may be responsible for the negative effects. Some researchers have claimed that the statistical methodology employed to determine the decline in semen quality was incorrect and that no real decline had taken place over the last decades. To investigate this claim, a group of researchers from the University Department of Growth and Reproduction and the Statistical Research Unit in Copenhagen Denmark, systematically
reviewed the complete international literature on semen analysis since the 1930’s using rigorous selection criteria and statistical analyses. They found, that linear regression of data weighted by the number of men in each study showed a significant decrease in mean sperm count from 113 X106/ml in 1940 to 66 X 106/ml in 1990 (p≤ 0.0001) and in seminal volume from 3.40 ml to 2.75 ml (p=0.027), indicating an even more pronounced decrease in sperm production than expressed by the decline in sperm density. They concluded, that there had been a genuine decline in semen quality over the last 50 years.48
The Danish study was subsequently also criticised with regard to the statistical methodology employed,49 but the issue would still not come to rest. A group of researchers from the MRC Centre for Reproductive Biology in Edinburgh, on the strength of the arguments against the statistical methodologies employed, regrouped the data to account for the year of the donor’s birth and found a similar decline in sperm concentration as reported by the Danish researchers,50 and all the trends seem to point to a decline in the health of the male reproductive system.51 It is true that a number of investigations, particularly with regard to the United States, have not shown a decline in semen quality,52,53,54 but overall the evidence is overwhelming that reproductive health is on the decline. An analysis of semen quality among fertile men in Paris using sperm stored in the sperm bank, showed that between 1973 and 1992 there had been no decline in semen volume, but that sperm concentration, motility and the percentage of morphologically normal spermatozoa had declined significantly.55
Of interest is also an observation that some nations experienced a greater decline than others in terms of semen quality a notable example being the comparison between Finland and Britain, where it has been reported that the British men are less fertile than those from Finland.56 Even in Finland, it has however been reported by researchers from the Forensic Department of the University of Helsinki, that the findings from post mortem analyses of two groups of men from 1981 and 1991 showed a dramatic decline in overall reproductive health. The researches reported that not only the number of men with normal spermiogenesis had declined by more than half, but the frequency of pathological disorders of the testes had increased.57 The precise reason for the overall decline, as well as differences between nations in reproductive health have not been clearly established. The main argument revolves around environmental oestrogens,58 but although this may be a contributing factor, even this hypothesis is still being considered as guesswork at this stage.59 The strongest evidence for the oestrogen argument is that the sons of women who were given high doses of diethylstilboestrol in the first trimester of pregnancy to prevent spontaneous abortions, have a high incidence of reproductive abnormalities.60 The main factors for male infertility are summarised in table 4.5.
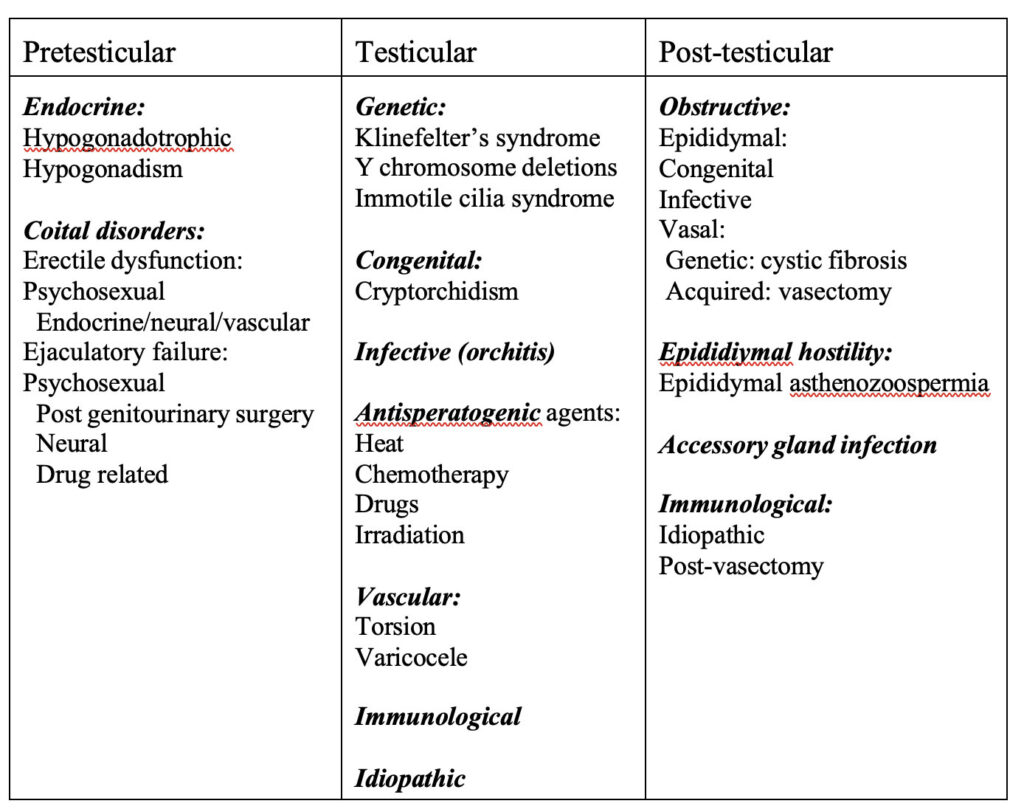
Table 4.5. Aetiological factors in male infertility. (From reference 61)
Although male infertility has received so much attention of late, female infertility is even higher than that of males. One couple in 10 seeks medical help because of infertility and a 1982-85 multicentre study by the World Health Organization found that in 20% of cases the problem was predominantly male, in 38% the problem was predominantly female, in 27% abnormalities were found in both partners and in the remaining 15% no clear-cut cause of infertility was identified.62 Although environmental pollutants and oestrogenic drugs may play a significant role in the decline in fertility, other factors, such as changes in diet, may be equally significant.
There have been significant changes in the consumption of animal products in Western societies over the last decades, and the consumption of dairy products in particular has increased dramatically. Fat consumption has also seen a significant increase in the past decades (see chapters 3 and 5) and these dietary changes have been associated with increased risk of degenerative diseases. Male prostate pathology has been linked to the consumption of dairy products,5 and this led us to investigate the possible link between the consumption of dairy products and reproductive health. The study was conducted on vervet monkey at the Primate Unit of the MRC in South Africa, so as to get as a close a model to the human as possible. Twelve monkeys were divided into two groups of six individuals each and they were put on diets containing 17% protein. The one group received largely maize and legumes and the other group milk powder as protein source. In order to assess the impact of high and low protein concentrations, after an initial two month period the protein allocation was
dropped to 8% from the respective sources and analyses were continued for an additional two month period. In this way the long- and short-term impact of the consumption of dairy products on reproductive health could be assessed. Already in the short-term, a significant decline in sperm quality, motility and concentration could be discerned, and these preliminary results were reported at the 6th International Congress on Cell Biology and 36th American Society for Cell Biology Annual Meeting held in San Francisco USA in 1996.63
When protein concentrations were high, the sperm concentrations between the two groups of monkeys were not significantly different, but progressive motility and the number of defective spermatozoa (particularly midpiece defects) increased. When protein concentrations were lowered to 8% crude protein, the group on dairy experienced a significant decline in sperm concentration, whilst the group on legume and maize showed no drop in sperm concentration and even showed an improved motility. Moreover, the number of defective spermatozoa also increased in the dairy group. In figures 4.10 and 4.11 the sperm progressive motility and the sperm concentration of the two groups of vervet monkeys is shown for the first four month period.
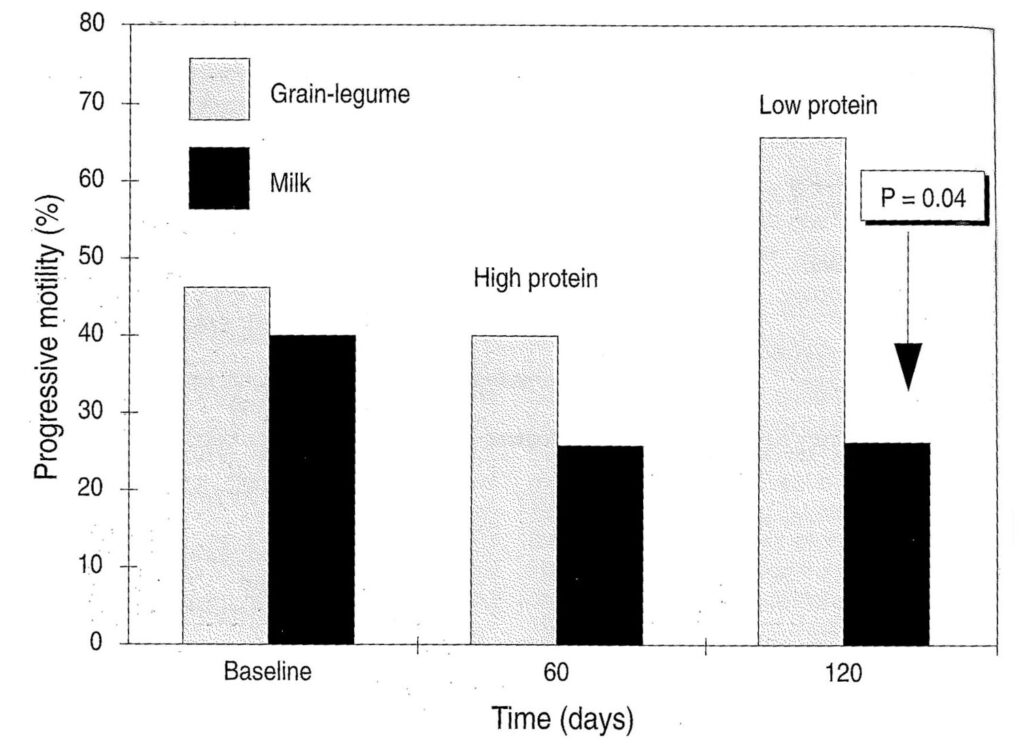
Figure 4.10. Progressively motile sperm of monkeys on milk and legume plus maize diets as protein source. (P=0.04 verified via the Wilcoxin 2-sample Test) The baseline represents the status of the animals at the start of the experiment before the introduction of the new dietary regime. (From reference 35).
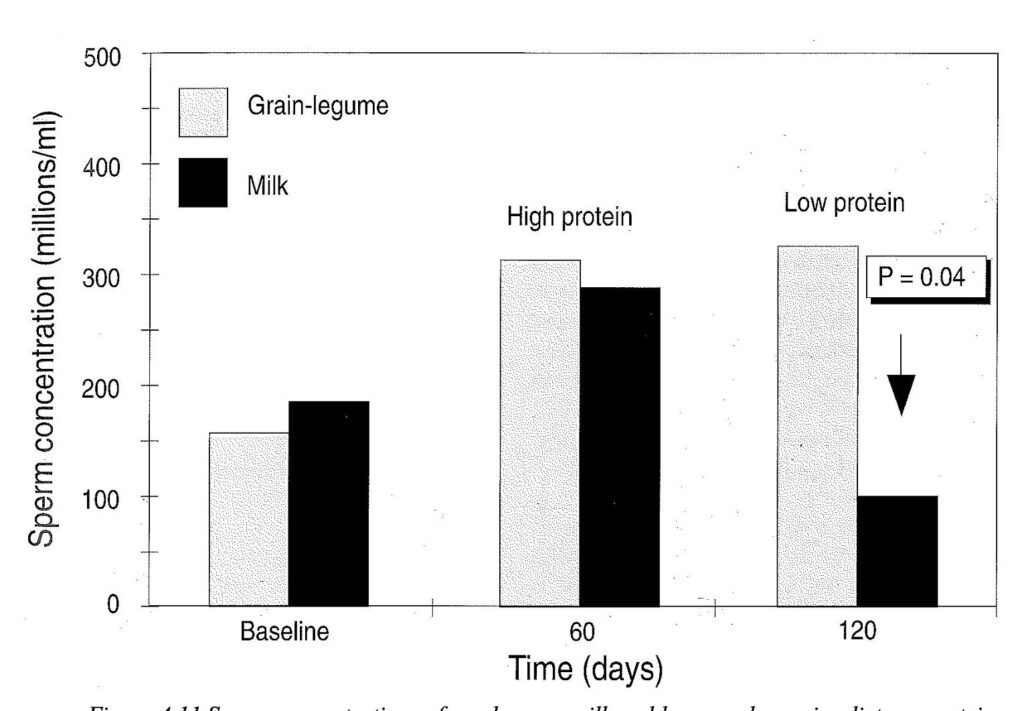
Figure 4.11 Sperm concentrations of monkeys on milk and legume plus maize diets as protein source. (P=0.04 verified via the Wilcoxin 2-sample Test) The baseline represents the status of the animals at the start of the experiment before the introduction of the new dietary regime. (From reference 35).
ANIMAL PRODUCTS AND FOODBORNE ILLNESS
Foodborne illness is on the increase worldwide and in most cases animal products are implicated as the main source of infection. These infections may be mild, seriously debilitating, and can even be fatal, particularly in elderly people and infants. The contamination of the food is due to micro-organisms or their toxins, and is characterized by diarrhoea, vomiting or both, but can also involve other parts of the body as in the case of listeriosis (caused by Listeria) or botulism which is caused by toxins produced by the bacterium Clostridium botulism. In the case of the latter, as little as 0,1g of food in which this bacterium has grown can be seriously debilitating, and in as many as 20% of cases botulism results in death. Most of the data pertaining to foodborne diseases is from the industrialized nations, but it must be borne in mind that the situation in poorer nations is probably worse.
The bacteria most often implicated with foodborne diseases are Salmonella, Campylobacter, Listeria, Eschericia, Staphylococcus and Yersinia.
Salmonella infections
Animals are the main source of this infection, but the infection can be spread from person to person. In the United States it is estimated that salmonellosis cases range from 790 000 to 3 690 000 per year, with as many as 7 041 deaths resulting from the illness.64 In the last two decades there has been a steady increase in the number of reported cases, and in industrialised countries a dramatic increase seems to have occurred since the mid 1980’s. In both the United States and Canada there has been a steady increase in salmonellosis and between 1975 and 1988 the incidence of notifiable diseases had more than doubled in these countries. Most outbreaks of the disease are associated with animal products such as eggs, cheese and improperly pasteurized milk. Between 1985 and 1989 there was also a steady increase in cases of Salmonella enteritidis in New England and the Mid-Atlantic states where there were 140 outbreaks (4 976 cases and 30 deaths) during this period in which eggs were associated with 65 of these outbreaks.65
Salmonella outbreaks in the UK have also been associated with infections in cattle and poultry, and increases in salmonellosis, since 1985 have been largely linked to a massive rise in cases caused by S. enteritidis attributed largely to poultry and hens’ eggs (figure 4.12).66 The eggs do not only become infected because of cracks in the shell, but they become contaminated because the ovarian tissue of the fowls is infected.
Prevention of contamination requires the co-operation of a wide variety of people from the breeders, veterinarians, epidemiologists, microbiologists and caterers, to every household cook. In view of this complexity it is difficult to control the spread of these diseases, particularly since transport and slaughter of animals increases the number of animals which carry Salmonella. In the UK the proportion of infected calves increases from 0,5% for calves leaving the farm to 36% after slaughter, whereas a US study found that in the case of pigs 7% are infected when they leave the farm, but 50% are infected after slaughter.66
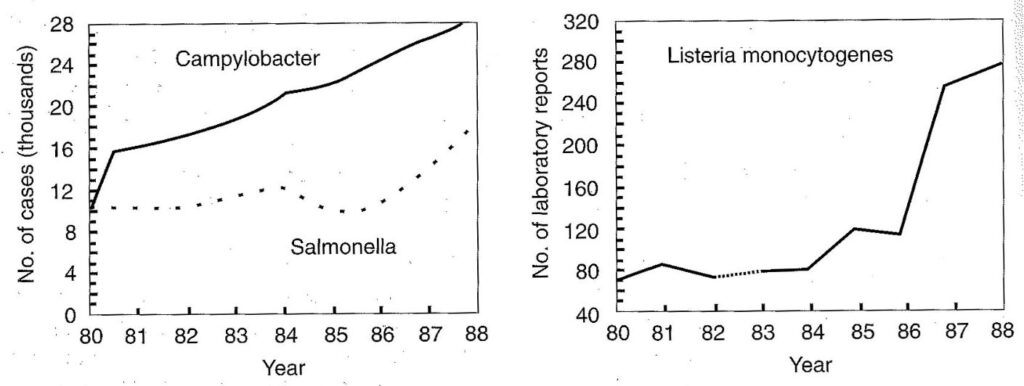
Figure 4.12. Cases of gastrointestinal infection due to bacterial contamination of food. (Adapted from reference 67)
Campylobacter infections
Campylobacteriosis is a common cause of sporadic disease associated mainly with poultry and milk. In Canada this micro-organism is responsible for more cases of infectious diarrhoea than is Salmonella, and in England and Wales it is the most common cause of this illness, with as many as 30 000 cases reported annually.67 Figure 4.12 shows that the incidence of this infection in the UK has also increased dramatically since 1980. In third world countries however the situation is much worse, and in African populations campylobacteriosis is very common.
Listeria infections
Listeria infections are not nearly as common as those caused by Salmonella or Campylobacter, but in view of the serious nature of the symptoms caused by these infections, it is imperative that this organism be strictly controlled. Listeria causes a range of symptoms ranging from mild flu to chronic septicaemia. It can result in abortion, stillbirth or the birth of severely affected babies.67 Listeriosis is caused by eating contaminated food, and in Canada it has claimed more lives than any other food-borne bacteria. The bacteria have been isolated from a wide range of dairy products such as milk, even pasteurized milk, chicken, and sea foods including fish. The bacteria have also been found in coleslaw and even black pepper. Bacterial contamination is also not uncommon in frozen and even pre-cooked chilled chicken.68 In Spain, Listeria spp. Were isolated from milk tanks on farms, and Listeria monocytogenes and L. Innocua were detected in 2.56 and 1.73% of the samples. Moreover, milk contamination by Listeria appeared to be seasonal, with a higher incidence in autumn and winter than in spring or summer and interestingly, the incidence was also lower on mountain farms than in plateau farms.69 Soft cheeses and pates are sometimes heavily infected and there has been a striking increase in disease cases in England and Wales since the mid-1980s (Figure 4.12) and also in North America where it was linked to “Mexican style” soft cheese. Outbreaks also occurred in Switzerland with more than 200 cases reported, and 91 deaths.66 In South Africa there was an outbreak of listeriosis in Soweto which claimed the lives of 43% of the fourteen detected cases. In Soweto alone, between two and four cases of this disease are reported annually. Listeria is particularly troublesome because it can continue to grow at refrigeration temperature.
Eschericia coli infections
Some strains of E. coli can cause intestinal infections. In the US cases of haemorrhagic colitis, haemolytic uraemic syndrome, and thrombotic thrombocytopenic purpura have been reported since 1982. Animal products are again implicated in these infections, and milk and beef are the main sources of infection.70 In May 1996, an epidemic of food poisoning rocked Japan, which the World Health Organization declared “unprecedented” in modern history. The outbreak started in Oku, a fishing village 180 km west of Osaka and spread to virtually every prefecture in Japan and effected more than 8000 people. The elderly and small children suffered most, and numerous deaths were reported. The infectious agent proved to be a particularly virulent strain (0157:H7) of E.Coli. In this case, animal products were once again implicated. Since 1992 enterohaemorrhagic E.coli have become the most frequent causative agent of haemorrhagic diarrhea in North America, and in Europe infections are also becoming more frequent. Unlike other E. Coli, enterohaemorrhagic E.coli possess cytotoxic shiga-toxins which previously were known only in cases of Shigella dysenteriae infections.71
Yersinia infections
Milk and other animal foods are a source of Yersinia enterocolitica which can cause acute gastroenteritis. In Belgium, Canada, the Netherlands, Australia and parts of Germany, infections from this organism are as common as Salmonella infections, and children in particular are vulnerable. The organism can grow at temperatures as low as 0°C and the increase in refrigeration practices may select for this organism.67
Other organisms
Staphylococcus aureus is becoming a frequent pathogen in hospital epidemics, and this is
particularly alarming, since there are a limited number of drugs to which this bacterium is susceptible. It is feared that antibiotic strains of this species could lead to widespread hospital epidemics, should such strains become more common.72 Other infectious micro-organisms that are transmitted by animal products include Clostridium perfringens which is found in meat. From 1986 to 1988 there has been a 46% reported increase of infected cases in the UK A further organism is Vibrio vulnificus which occurs in oysters and has been implicated in infections in the U.S.A.67
MODERN ANIMAL HUSBANDRY
Animal husbandry has numerous facets, and great changes in farming practices as well as an enormous expansion in the pharmaceutical industry, have changed the face of the animal-products industry over the past decades. Particularly the use of drugs has had a profound influence on animal husbandry. Drugs are not only used to curtail disease but they are also extensively used to stimulate growth, and this last factor has led to an unprecedented increase in the use of drugs.
Antibiotics
Antibiotics have had a profound effect on the agricultural sector, and today antibiotics are used extensively in animal husbandry. Antibiotics are not only administered to animals for the treatment of disease, but subtherapeutic doses of these antimicrobials are administered routinely for growth promotion in livestock and poultry production. Antibiotics are also used in wildlife and fish, and for the control of plant diseases and food spoilage. In the United States alone some 15 million pounds of antibiotics are administered to farm animals annually. The fact that animals grow faster when receiving subtherapeutic doses of antimicrobials serves as an incentive to farmers to administer these products, particularly since an added benefit is found in disease prevention. Although vehemently denied in some quarters, this practice is giving rise to a new generation of antibiotic-resistant microbes which can cause serious outbreaks of disease among humans. Infectious diseases account for millions of deaths annually, with respiratory infections, diarrhoeal diseases and tuberculosis accounting for the majority of these.
Drug-resistant bacteria have accounted for a steady increase in the incidence of human Salmonella infections,73 and in 1983 an outbreak of Salmonella infection in the Midwestern states of the USA was actually traced to the farmyard from which the disease spread.74 An epidemiologic investigation in Minnesota revealed that patients had eaten ground beef (hamburger) and that the meat had come from a farm lot where the cattle had been fed subtherapeutic quantities of chlortetracycline for growth promotion and disease prevention.
In outbreaks of gastrointestinal disease from drug-resistant bacteria, it is a common occurrence that infected patients had taken antibiotics for other diseases such as bronchitis, pharyngitis, otitis media (ear infection) or other non-diarrhoeal diseases prior to the onset of the gastrointestinal disease. This suggests that whilst patients are on antibiotics, and they consume foods infected with resistant bacteria, the destruction of the natural non-resistant intestinal bacteria offers some selective advantage to the drug-resistant varieties which then flourish and become pathogenic. The symptoms are normally diarrhoea, abdominal cramps, nausea and vomiting and in some cases chills, fever, and confusion. Furthermore, the disease is difficult to treat, as the bacteria will not respond to drugs in view of their antimicrobial resistance, and death can be the ultimate result, even in hospitals with all the necessary care
facilities.
The fact that antibiotics are widely used in hospitals, accounts for the fact that outbreaks of antimicrobial-resistant bacterial infections are largely recorded in these institutions. Bitter rows have developed over this issue between governments and trade organizations. In Germany and Denmark the antibiotic avoparcin, which farmers inject into their livestock, was banned because of concern that antibiotic resistance could spread from the farmyard to hospitals. Brussels, on the grounds that the ban could interfere with free trade, declared the ban illegal. Avoparcin is similar to other antibiotics such as vancomycin and teicoplanin which are the only drugs available that kill methicillin-resistant Staphylococcus aureus (MRSA), which is becoming more and more prevalent in hospitals. Microbiologists were dismayed that the German studies had not been able to uphold the ban.72 Sadly it is often the elderly or infants who succumb to the disease due to their weaker constitution.
In view of the widespread use of antibiotics in animal husbandry, the most common sources of contamination, by this new breed of antibiotic resistant bacteria, are poultry, cattle, calves, eggs and milk. In fact, in over two thirds of US outbreaks of multiple drug-resistant Salmonella infections with a definite source, the bacteria came from food animal populations, and the transmission of resistant bacteria to man, through the consumption of food animals, is thus not a rare event.75 The World Health Organization has reported that resistant strains of Salmonella typhimurium have increased dramatically in many countries, and there was hardly any medication that was effective against the DT 104 strain of this species. In some European countries the total number of Salmonella infections has increased 20 fold in the last decade and in Britain, where DT 104 was first isolated in 1988, the number of infections from this strain increase from 300 in 1990 to 3 500 in 1996. In Germany, the percentage of infections caused by this strain rose from ten to 18% within the year 1996 alone.76
Tetracyclines are the most commonly used antibiotics in feeding operations, and these drugs commonly occur in the animal products purchased from supermarkets and other stores. Contamination of foods with antibiotics may present various health hazards and can be strongly allergenic in sensitive individuals. A study on the occurrence of antibiotic residues and drug-resistant bacteria in beef and chicken tissues purchased from supermarkets in Hermisillo, Mexico, showed that 86% of beef samples were contaminated with streptomycin whilst other antibiotics were also prevalent. Chicken breasts sampled, likewise, showed high levels of contamination which exceeded FDA tolerance limits (Table 4.6).77
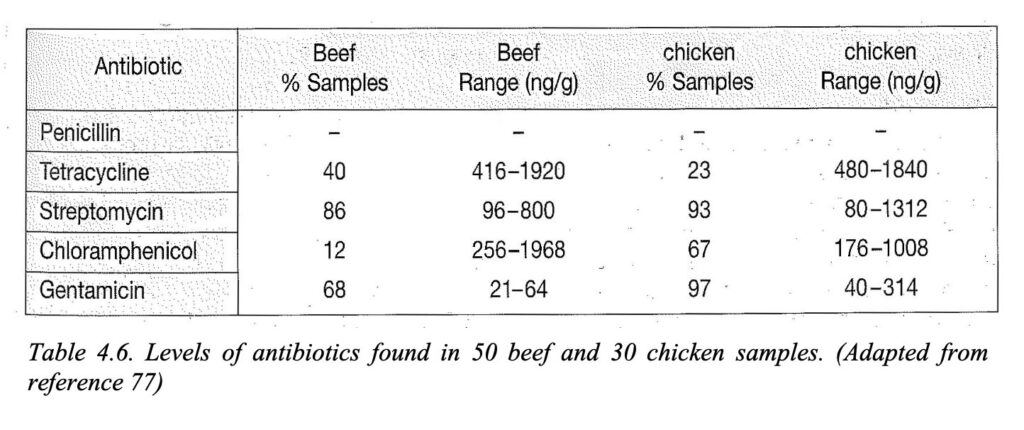
Table 4.6. Levels of antibiotics found in 50 beef and 30 chicken samples. (Adapted from reference 77)
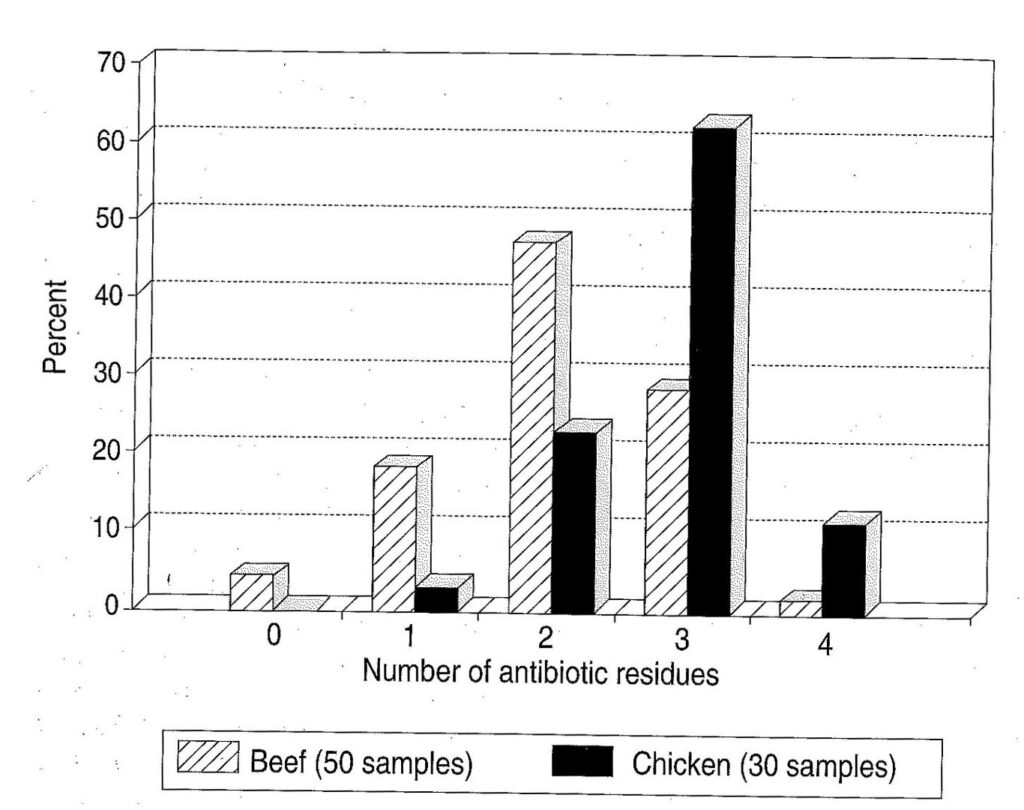
Figure 4.13. Number of antibiotics detected in beef and chicken samples. (Adapted from reference 77)
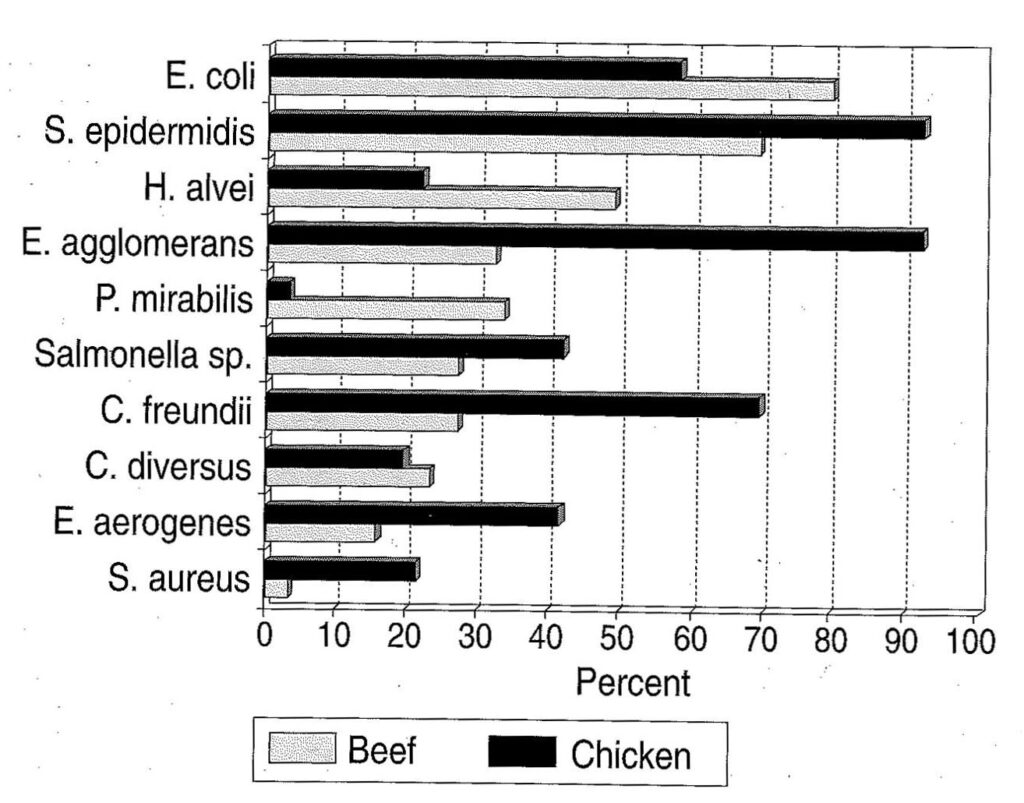
Figure 4.14. The frequency of microorganisms isolated from beef and chicken samples. (Adapted from reference 77)
In this study it was found that in more than 50% of the chicken and beef samples investigated, more than one antibiotic was present at the same time, and in some cases three or four different antibiotics had been administered to the animals simultaneously (Fig. 4.13). The frequency at which the different micro-organisms occurred in the samples varied, but a wide range of potentially pathogenic species was prevalent in both beef and chicken samples (Fig 4.14).
From table 4.7 it is evident that no penicillin was found in any of the samples investigated. The reason for this is that penicillin is no longer used subtherapeutically in these areas as it has become ineffective. Bacteria resistant to penicillin were however isolated from these tissues, showing that drug resistance persists beyond the time in which the drugs were used. Nearly all the bacteria isolated from the above mentioned tissues were resistant to penicillin, with high resistance to tetracycline and streptomycin also noted (Table 4.7).
In view of the current controversy surrounding the issue of antibiotic resistant bacterial strains, two questions seem vital at this stage:
- Is the use of subtherapeutic doses on farms responsible for the increase in resistant strains?
- What is the status regarding vancomycin resistance?
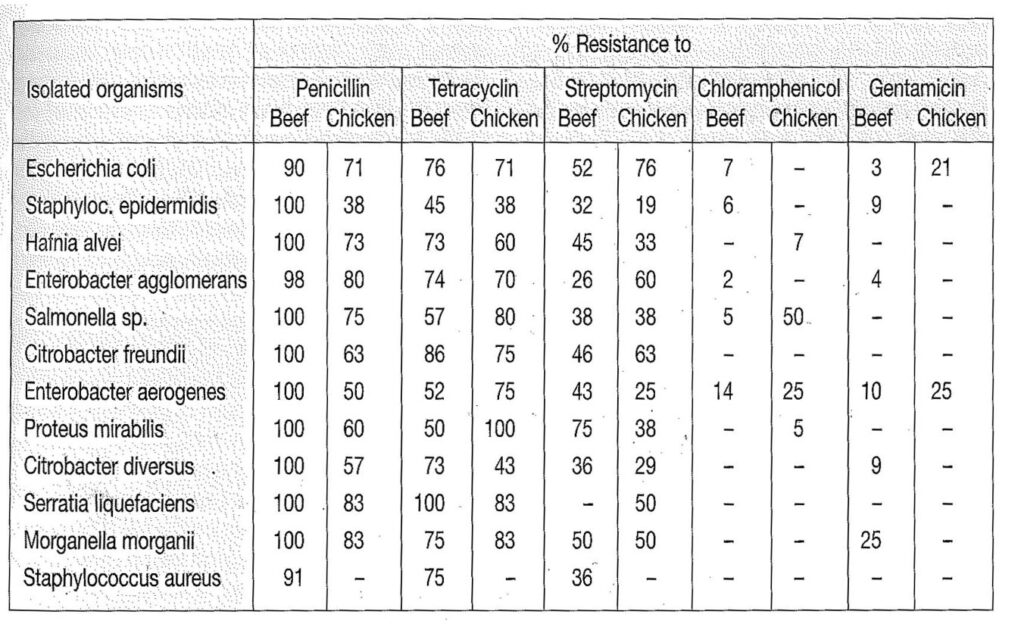
Table 4.7 Antibiotic resistance in bacteria isolated from 50 beef and 30 chicken samples. (Adapted from reference 77).
The argument by industry has been that subtherapeutic doses cannot enhance resistance, however, this does not seem logical as even low doses of antibiotics should provide a selective advantage to resistant strains. If indeed this is the case, then at least certain antibiotics should be banned for use in the animal husbandry industry. Vancomycin is a case in point, as vancomycin is the only drug that can kill methicillin-resistant Stapylococcus aureus which is causing hospital epidemics with alarming regularity.72 To examine this issue, a project was jointly undertaken by the Departments of Zoology and Microbiology at the University of the Western Cape, in which chicken, pork, beef and milk samples were tested for bacterial contamination and multiple antibiotic resistance in the greater Cape Town area. Animal bacterial samples were taken at abattoirs and at retail outlets, the rationale being that differences in resistance between the two groups of samples should pinpoint the source. Higher resistance levels in abattoir samples taken at the beginning of the slaughtering cycle would indicate that the resistance had emanated from the farm. The results for the chicken samples have thus far been evaluated, and are presented in table 4.8.
The results clearly show that a large proportion of the bacterial strains showed multiple antibiotic resistance, and in most cases the bacteria from the abattoir samples had a higher resistance to antibiotics than the retail samples thus indicating that the resistance route came via the farm. The very high resistance levels displayed by most of the bacteria is certainly unsettling. Staphylococci were resistant to tetracycline and oxacillin but the percentage of abattoir isolates that displayed simultaneous resistance to both tetracycline and oxacillin was nearly double that of retail samples (69.6% versus 39.4%).Gram positive bacteria (Staphylococcus) are susceptible to vancomycin, and although resistance of Staphylococcus to vancomycin as well as methicillin was not very high, even the 7% resistance recorded in retail samples is cause for concern, considering that this is the only drug that can kill methicillin-resistant Staphylococcus aureus.78
Producers are required to observe a withdrawal period after administering antibiotics, prior to marketing their product. It is, however, not feasible to monitor all the meat that goes to market, and studies on swine have shown that producers do not adhere to the specified withdrawal times.79 Antibiotic residues are even found in carcasses of cattle with no record of antibiotic treatment.80 Even if they should adhere to these withdrawal times, it is doubtful whether this will be of much benefit, considering the fact that resistance has been maintained over years to antibiotics that are no longer in use. Besides the antibiotic problem, contamination of carcasses with antimicrobial agents and other dangerous compounds such as heavy metals, organochlorine compounds, organophosphorous compounds and growth stimulants, is now so widespread that methods are being devised to routinely monitor these contaminants in the interest of human safety.81
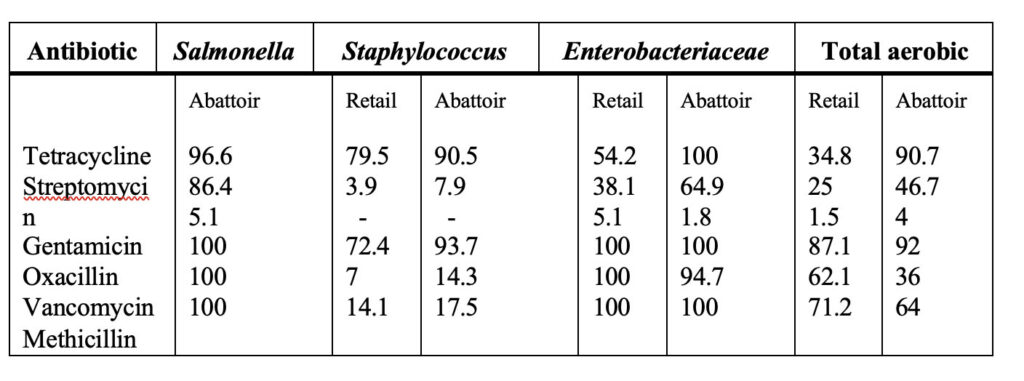
Table 4.8. Percentage resistance of various retail and abattoir chicken isolates to six antibiotics. (From reference 78)
Additional growth promoters
Besides the addition of antimicrobials to promote growth, animal feed is also routinely spiked with hormonal growth promoters of which some may be carcinogenic. Hormone residues that have been isolated from beef include trenbolone acetate, zeranol and stilbene diethylstilboestrol (DES), oestradiol, dienoestrol, hexaestrol, 17α-ethynyloestradiol, ketosteroids, testosterone, progesterone and progesterone acetate, which are all used as anabolic steroids to promote weight increase. To promote lean meat production, animals are fed β-agonists, a group of drugs that convert fats to fatty acids and stimulate the formation of proteins, to promote rapid weight gain. In addition in some countries growth hormone is administered and even genetically-engineered hormones are used, such as PST, which is used
to promote lean meat production in pigs. Some of these growth promoters, such as clenbuterol, are banned, but there is a healthy black market trade in these growth-promoting drugs as shown by the clenbuterol scandal in 1996 when German authorities found that the drug was being used on more than 40 calf fattening farms in Nordrhein-Westfalen and consequently prohibited the slaughter of 2400 calves and arrested a veterinary drug dealer. In a further case around the county of Gütersloh, calves were found with the banned antibiotic Chloramphenicol.82
Farm animals today are often treated as commodities, like inanimate consumer goods. They are frequently housed in unhealthy environments and fed virtually anything that will promote growth and increase profits, even though the long-term effect on the health of the animals or the human consumer is not known. In large chicken hatcheries the chicks never see sunlight, but are subjected to low-intensity light for close on 24 hours per day. The lights are switched off only for approximately 15 min each day so that the chickens can get used to darkness, lest they panic during a power failure and cause production losses. Animals are cramped together to limit their movements and energy expenditure, because growth and mass increase are the paramount criteria that are taken into account when designing these facilities. New breeds of chickens are selected for growth performance with virtual disregard for all other parameters. In the past, a free range chicken could be assumed to consume approximately 17kg of feed to grow to a market mass of 1.5kg. Today, some breeds utilise only 3.5kg to achieve the same mass increase, and this in only six weeks. The chickens are geared for rapid growth, but their other systems are severely compromised. The cardiovascular system, internal organs and immune systems are poorly developed so that extreme care must be taken not to induce stress or exposure to infectious bacteria lest they die before reaching market size.
Farm animals are fed carcass meal, fish meal, edible plastic, sewage, petro-chemical residues and excrement. On some farms veritable food chains have been set up where chicken manure, from battery chickens, is fed to the sheep and cattle, and dead chicks and unhatched eggs in turn are the feed items used in the piggery. In the chicken industry, the slaughter offal such as entrails, legs and heads are often dried, ground and recycled as feed , thus effectively turning the chickens into cannibals. Moreover, the chickens are routinely manipulated with a host of growth stimulating, antimicrobial and digestibility enhancing drugs.
Prion diseases
Prions cause a group of animal and human neurodegenerative diseases which are now classified together because of their etiology and pathogenesis. The infectious agent is not a virus, nor does it contain DNA sequences, it is a brain protein which has undergone modification. Prion proteins are thus thought to exist in two forms, the benign Prion protein (PrPc)and the infectious ‘scrapie form’ (PrPSc).83,84 The normal Prion protein consists of strands of amino acids twirled into helices whereas in the infectious form the amino acid strands are flattened into β-sheets which can cause transmissible dementias. Transmissible dementias are degenerative conditions associated with neuronal loss, and neuronal vacuolation or spongiform (spongy) changes. Furthermore, the changes are accompanied by the accumulation of the abnormal proteinase-resistant prion protein known as PrPSc which has undergone posttranscriptural changes, and the ensuing disease is thus termed a prion disease .
Prion disease is becoming a high-profile public health issue, particularly since the Bovine Spongiform Encephalitis (BSE) or “mad cow’s disease” epidemic rocked Britain. Beginning in 1986, this previously unknown prion disease decimated the beef industry in Britain and it has been proposed that some 160 000 cattle were affected. The infectious agent
was probably transferred to the animals by routinely feeding them meat and bone meal dietary supplements. Carcass meal is predominantly prepared from animals that have died of disease, or animals that have been condemned at the abattoir as unfit for human consumption. The carcass meal and excrement is heat-sterilized to kill the bacteria, but recently chemical sterilization has become the method of choice in many countries, as it is cheaper. Since 1988 the feeding of dietary protein supplements derived from sheep or cattle offal has been banned in Britain and it is argued, that this step has brought the epidemic under control. The incidence of reported cases has indeed declined since the peak was reached in 1992 (figure 4.15).
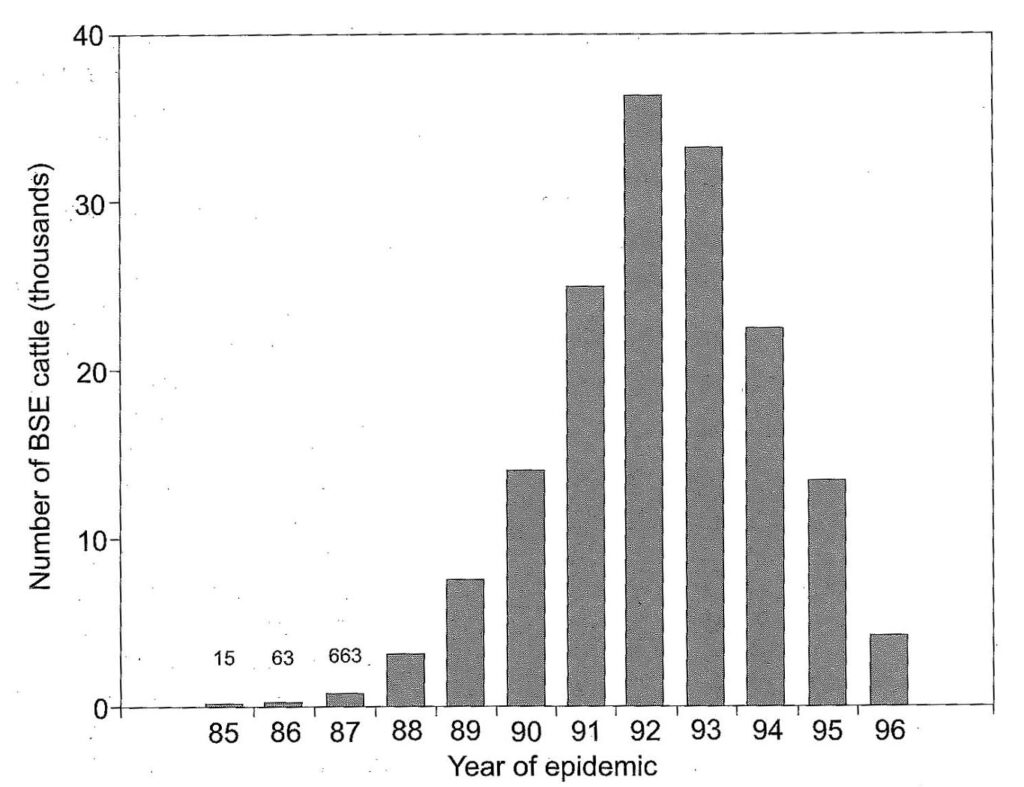
Figure 4.15. The number of bovine spongiform encephalopathy cases reported in Great Britain during the epidemic. (Adapted from references 83, 85).
Spongiform encephalopathies are transmissible dementias, and occur in man as Creutzfeldt-Jacob disease (CJD), Gerstman-Straussler syndrome, and kuru. In other animals it occurs as scrapie in sheep and transmissible mink encephalopathy in ranch mink. In the UK alone some 75 000 people per year die demented, of which 50% have Alzheimer’s disease and 2% have Creutzfeldt-Jacob disease.86 The latter disease is characterized by a sudden onset of disease, with rapid progression through dementia and death within a year.87 Economic pressures led to initial denials that consumption of BSE contaminated beef could lead to Creutzfeldt-Jacob disease, but in 1996, after a decade of ministerial denials the British Government reluctantly admitted the link between the two.88,89 Since this time, European governments have reacted strongly, banning British beef90 and even slaughtering thousands of head of cattle to restore consumer confidence. In Switzerland the government subsidized the slaughter of 230 000 cows born before 1 December 1990 to restore faith in Swiss beef.91
Prior to the admission that there was a link between BSE and CJD it was argued, that cross species contamination was not possible and that one could not contract the disease from eating contaminated food. However, instances of exotic animals in captivity with transmissible dementias have been linked to consumption of meat and bone meal, and instances in domestic cats in the UK are assumed to be due to BSE-infected offal in cat food.92 In early 1996 it was recognized that the new variant of CJD that was affecting 12 young persons in the UK had been transmitted via BSE contaminated beef. The experimental transmission of the disease by inoculating macaques (Old World monkeys) with BSE infected brain homogenate proved that cross species transmission was possible,93,94 and it is now even well established that transmission occurs between infected cows and their calves thus raising questions about the future of the epidemic.95,96,97
It has been argued, that what happened in Britain is but the tip of the iceberg, and that major epidemics could erupt worldwide. Thousands of Europeans could be unknowingly infected with the disease and could die, and even in the US some researchers feel that the conditions which led to the UK outbreak can lead to similar events in the USA.98. Statistics already suggest, that BSE is now Europe-wide and by May 1996 Switzerland had reported 211 cases of BSE, Eire 125, France 18, Portugal 30, whilst a total of 71 706 tonnes of British meat and bone meal and 33 424 breeding bovines have been exported to EU member states from 1985 to 1990.99 Even if infection of new animals ceases, it has been predicted that between 15 000 and 24 000 new cases of BSE would occur between 1996 and 1999.100
Mycotoxins
Regulations regarding animal feeds are not as stringent as those regarding food for human consumption, and feed that is contaminated with mycotoxins can be a further source of disease if fed to farm animals. Mycotoxins are toxins produced by fungi, and contaminated foodstuffs is a major problem in most tropical and subtropical countries. Aflotoxins are fungal toxins produced by Aspergillus flavus, A. parasiticus and Penicillium puberculum, and constitute a serious world-wide problem. Aflotoxins contaminate peanuts, nuts, rice, grains, soya beans, peas and sorghum seeds, all of which can end up as animal feed. Aflotoxins AFM and AFM2 are hydroxylated metabolites of the aflotoxin AFB and AFB2, which are the most potent liver carcinogens in rats, producing 100% incidence of liver tumours in rats at a dosage of 95µg/kg. These aflotoxins have been found in liver, milk, blood and kidneys of animals fed aflotoxin-contaminated feeds.12 Orchatoxin-A, another potent carcinogen, is produced by Penicillium, and has been found in cereals and meat products at levels of 1035µg/kg.
Contamination of the animals does not end at the farmyard, but continues in the slaughterhouses of the world. Abattoirs are concerned with speed rather than the well-being of the animals, and stress and terror are endemic.74 Carcasses are contaminated by faecal bacteria when they come into contact with ruptured intestines or fall on the ground. Because of contamination with the faecal bacteria Yersinia enterocolitica, Campylobacter spp., Salmonellae and Aeromonas hydrophila, as well as residues of veterinary drugs and mycotoxins, it has even been suggested that carcasses be decontaminated by radiation to combat the health hazards.101
Genetic engineering
Genetically engineered livestock is expected to revolutionize the agricultural industry. It is envisaged that animals can be made to grow faster and to incorporate changes in fat composition so as to be more suitable for human dietary needs. Gene transfers have been carried out on laboratory animals, but have also recently been extended to domestic animals. Most studies have centred around growth-regulation, as studies in mice have shown that gene transfers of bovine, ovine, rat or human growth-hormone genes can almost double the rate of growth in mice. Transgenic farm animals already include chickens, cows, pigs, sheep, rabbits and fish. Human, Bovine and rat growth-hormone genes have been transferred to pigs, but the mortality rates in these animals is high. Leaner meat has been produced in transgenic pigs, but at a price.
Transgenic animals suffer from a variety of pathological changes which shorten their lifespan. In pigs it was found that the animals were lethargic, and suffered from lameness, uncoordinated gait, protruding eyeballs and thickened skin. Moreover, they suffered from gastric ulceration, severe synovitis, degenerative joint disease, pericarditis and endocarditis, cardiomegaly, parakeratosis, nephritis and pneumonia.102 The risk of disease from contaminated animal products today is indeed something to consider. In the past the major concerns revolved around infectious diseases and parasitic and viral infections. This risk still exists today, but additional risk factors have been added through modern animal husbandry.
Modern technology has also had its effect on plant foods, with gene transfers being currently in vogue. The long term effects of these manipulations are also not known and these products may also be viewed with some degree of scepticism. However, man has to eat, and if a choice has to be made between manipulated plant or animal foods, the consumption of plant foods would certainly be associated with lower risks of contracting diseases. A diet free from animal products, and concentrating on a variety of fresh whole foods will supply excellent nutrition and will at the same time protect against many of the modern ills associated with Western diets. Such a diet need not, and indeed should not, be less attractive than a diet based on animal products. A little ingenuity with emphasis on variety will provide an exciting, healthy lifestyle.
REFERENCES
- Parkin, D.M. et al. 1992. In:Bingham, S.A. Epidemiology and mechanisms relating diet to risk of colorectal cancer. Nutrition Research Reviews (1996), 9:197-239.
- Bingham, S.A. 1996. Epidemiology and mechanisms relating diet to risk of colorectal cancer. Nutrition Research Reviews, 9:197-239.
- Muir, C. Et al. 1987. In:Bingham, S.A. Epidemiology and mechanisms relating diet to risk of colorectal cancer. Nutrition Research Reviews (1996), 9:197-239.
- Armstrong, B. And Doll, R. 1975. Environmental factors and the incidence and mortality from cancer in different countries with special reference to dietary practices. International Journal of Cancer. 15:617-631.
- Snowdon, D.A. 1988. Animal product consumption and mortality of all causes combined, coronary heart disease, stroke, diabetes and cancer in Seventh-day Adventists. Am. J Clin. Nutr. 48:749-53.
- Snowdon, D.A., Phillips, R.L. 1985. Does a vegetarian diet reduce the occurrence of diabetes? Am J. Public Health 75: 507-12.
- Mc Burney, M.I., Horvath, P.J., Jeraii, J.L., Van Soest, P.J. 1985. Effect of in vivo fermentation using human faecal inoculum on the water holding capacity of dietary fibre. Br
J. Nutr. 53: 17-24
- Ames, B.N and Gold, L.S. 1990. Too many rodent carcinogens: Mitogenesis increases mutagenis. Science 249: 970-971.
- Bone, E., Tamm, A., and Hill, M. 1976. The production of urinary phenols by gut bacteria and their possible role in the causation of large bowel cancer. Am.J.Clin.Nutr. 29:1448-1454.
- Cummings, J.H., Hill, M.J., Bone, E.S., Branch, W.J., Jenkins, D.J.A. 1979. The effect of meat protein and dietary fibre on colonic function and metabolism. II Bacterial metabolites in feces and urine. Am. J. Clin. Nutr. 32: 2094-1011
- Obana, H., Hori, S. and Kashimoto, T. 1981. Determination of polycyclic hydrocarbons in marine samples by high-performance liquid chromotography. Bulletin of Environmental Contamination and Toxicology 26: 613-620.
- Tricker, A.R. and R. Preussmann. 1990. Chemical food contamination in the initiation of cancer. Proc. of the Nutritional Society 49: 133-144.
- Bingham, S.A. 1988. Meat, starch and nonstarch poly-saccharides and large bowel cancer. Am.J. Clin. Nutr. 48: 762-7.
- Sugimara, T. 1985. Carcinogenicity of mutogenic hetero-cyclic amines formed during cooking process. Mutation Research 150: 33-41.
- Overvik, E., Kleman, M., Berg, I., Gustafsson, J.A. 1990. Influence of creatine, amino acids and water on the formation of the mutagenic heterocyclic amines found in cooked meats. Carcinogenesis 10 (12) 2293-2301.
- Bartsch, H and Montesano, R. 1984. Relevance of nitro-soamines to human cancer
Carcinogenesis 5: 1381-93.
- Bingham, S.A., Pignatelli, B., Pollock, J,R.A., Ellul, A., Malaveille, C., Gross, G., Runswick, S., Cummings, J.H., and O’Neill, I.K.O. 1996. Does increased endogenous formation of N-nitroso compounds in the human colon explain the association between red meat and colon cancer? Carcinogenesis. 17 (3): 515-523.
- F. Pearce. 1996. Dead dolphins contaminated by toxic paint. New Scientist, 13 January 1996.
- F. Pearce. 1995. Dead in the water. New Scientist. 4 February, 1995.
- Editorial. 1991. Lactose intolerance. Lancet. 338:663-664.
- Levine, B. 1996. Most frequently asked questions about lactose intolerance. Nutrition Today. 31 (2) March/April 1996.
- O’Keefe, S.J.D., O’Keefe, E.A., Burke, E., Roberts, P., Lavender, R. and Kemp, T. 1991. Milk-induced malabsorption in malnourished African patients. Am.J.Clin.Nutr. 54:130-5.
- Carroll, K.K. 1991. Review of clinical studies on cholesterol-lowering response to soy protein. J.Am.Diet.Assoc. 91:820-827.
- Van der Meer, R., Beynen, A.C. 1987. Species-dependent responsiveness of serum cholesterol to dietary protein. J.Am.oil Chem.Soc. 64:1172-1177.
- Weaver, C.M., Heany, R.P., Martin, B.R., Fitzsimons, M.L. 1991. Human calcium absorption from whole-wheat products. J.Nutr. 121:1769-1775.
- Blank, R.P., Diehl, H.A., Ballard, G.T., Melendez, R.C. 1987. Calcium metabolism and osteoporotic ridge resorption: A protein connection. J.Prosthetet.Dent. 58:590-595.
- Howe, J.C. 1990. Postprandial response of calcium metabolism in postmenopausal women to meals varying in protein level/source. Metabolism. 39:1246-1252.
- Kitano, T., Esashi, T., Azami, S. 1988. Effect of protein intake on mineral (calcium, magnesium, and phosphorus) balance in Japanese males. J.Nutr.Sci.Vitaminol. 34:387-389.
- Kok, D.J., Iestra, J,A., Doorenbos, C.J., Papapoulos, S.E. 1990. The effect of dietary excesses in animal protein and sodium on the composition and the crystallization kinetics of calcium oxalate monohydrate in urines of healthy men. J.Clin.Endocrinol.Metab. 71:861-867.
- Howe, J.C. 1985. Effect of dietary protein, calcium and phosphorus on calcium metabolism in humans, in Kies C (ed): Nutritional Bioavailability of calcium. Washington, DC, American Chemical Society., pp 125-139.
- Greger, J.L., Krzykowski, C.E., Khazen, R.R., Krashok, C.L. 1987. Mineral utilization by rats fed various commercially available calcium supplements or milk. J.Nutr. 117:717.
- Bailie, I.E. 1987. Osteoporosis and `affluent diet’. Hospital practice. April 15, p16.
- Specker, B.L., Vieira, N.E., O’Brie, K.O., Ho, M.L., Heubi, J.E., Abrams, S.A., Yrgey,
A.L. 1994. Calcium kinetics in lactating women with low and high calcium intakes. Am.J.Clin.Nutr. 59:593-9.
- Prentice,A. Jarjou, L.M.A., Cole, T.J., Stirling, D.M., Dibba, B. Fairweather-Yait, S. 1996. Calcium requirements of lactating Gambian mothers: effects of a calcium supplement on breast-milk calcium concentration, maternal bone mineral content, and urinary calcium excretion. Am.J.Clin.Nutr 62:58-67.
- Johnson, Q. 1997. The effect of dairy consumption on reproductive health and other parameters of vervet monkeys. Ph.D. dissertation. (In prep)
- Isolauri, E. 1996. Studies on Lactobacillus GG in food hypersensitivity disorders.
Nutrition Today. Suppl. 31(6) November/December 1996
- Buisseret, P.D. 1978. Common Manifestation of Cow’s milk Allergy in Children. Lancet, Vol.1 Feb. 11 P304-305.
- Gerard, J.W. 1967. Milk Allergy: Clinical Picture and Familial Inudience. Canadian Medical Association Journal Vol 97 Sept 23 P 780.
- Murray, A.B 1986. Infant Feeding and Respiratory Allergy. Lancet Vol.1 Mar. 6 P497.
- Werfel, T., Ahlers, G., Schmidt, P., Boeker, M., Kapp, A., Neumann, C. 1997. Milk- responsive atopic dermatitis is associated with a casein-specific lymphocyte response in adolescent and adult patients. J.Allergy Clin.Immunol. 99:124-133.
- Ellis, T.M., and Atkinson, M.A. 1996. Early infant diets and insulin-dependent diabetes.
Lancet 347:1464-1465.
- Cavallo, M.G., Fava, D., Monetini, L., Barone, F., Pozilli, P. 1996. Cell-mediated immune response to β-casein in recent-onset insulin-dependent diabetes: implications for disease pathogenesis. Lancet 348:926-928.
- Harrison, L.C.. 1996. Cow’s milk and IDDM. Lancet 348:905-906.
- Fukushima, Y. Kawata, Y., Onda, T., Kitagawa, M. 1997. Consumption of cow milk and egg by lactating women and the presence of β-lactoglobulin and ovalbumin in breast milk. Am.J.Clin.Nutr 65:30-35.
- Jakobson, I., Lindberg, T. 1978. Cow’s milk as a cause of infantile colic in breast-fed infants. Lancet. August 26, 1978. pp 432-439.
- Truelove, S.C. 1961. “Ulcerative colitis provoked by milk. British Med. J. 1:154-165.
- Lucas, A., Morley, R., Cole, T.J., Lister, G., Leeson-Payne, C. 1992. Breast milk and subsequent intelligence quotient in children born preterm. Lancet. 339:261-264.
- Carlsen, E., Giwercman, A., Keiding, N. Skakkebaek N.E. 1992. Evidence for decreasing quality of semen during past 50 years. BMJ 305:602-613.
- Farrow, S. 1994. Falling sperm: fact or fiction? BMJ 309:1-2.
- Irvine, D.S. 1994. Falling sperm quality. BMJ 309:476
- Skakkebaek, N.E., Keiding, N. 1994. Changes in semen and the testis. BMJ 309:1316- 1317.
- Fish, H., Goluboff, E.T., Olson, M.S.T., Feldshuh, J., Broder, S.J., Barad, D.H. 1996. Semen analyses in 1 283 men from the United States over a 25-year period: no decline in quality. Fertility and Sterility 65 (5):1009-1014.
- Paulsen, C.A., Berman, N.G., Wang, C. 1996. Data from men in greater Seattle area reveals no decline downward trend in semen quality: further evidence that deterioration of semen quality is not geographically uniform. Fertility and Sterility 65 (5):1015-1020.
- Mc Carthy, M. 1996. US studies find no decline in sperm counts. Lancet 347:1319-1502.
- Auger, J., Kunstman, J.M., Czyglik, F., Jouannet, P. 1995. Decline in semen quality among fertile men in Paris during the past 20 years. N Engl J Med 332:281-285.
- Joffe, M. 1996. Decreased fertility in Britain compared with Finland. Lancet 347:1519- 1522.
- Ärzte Zeitung. 1997. Immer mehr Männer mit Spermiogenese-Störung.Ärzte Zeitung 15. Januar. 1997.
- Sharpe, R.M., Skakkebaek, N.E. 1993. Are oestrogens involved in falling sperm counts and disorders of the male reproductive tract? Lancet 341:1392-1395.
- The Lancet editorial 1995. Male reproductive health and environmental oestrogens.
Lancet 345:933-935.
- Stillman, R.J. 1982. In utero exposure to diethylstilboestrol: adverse effects on the reproductive tract and reproductive performance in male and female offspring. Am J Obstet Gynecol 142:905-921.
- Kretser,D.M. 1997. Male infertility. Lancet 349:787-790.
- World Health Organization. 1987. Towards more objectivity in diagnosis and management of male infertility. Int. J Androl 79Suppl):1-53.
- Johnson, Q. Veith, W.J., van der Horst, G. Seier, J. 1996. The impact of dietary protein on testosterone production and sperm quality in male vervet monkeys. Abstract H160. 6th International Congress on Cell Biology & 36th American Society for Cell Biology Annual Meeting, San Francisco, December 11, 1996.
- Talami, R., La Vecchia, C., Decartli, A., et al. 1984. Social factors, diet and breast cancer in a northern Italian population. Br.J.Cancer. 49:723-9.
- Todd, E. 1990. Epidemiology of foodborne illness: North America. Lancet. 336:788-790. 66.Waittes, W.M and Arbuthnott, J.P. 1990. Foodborne illness: an overview. Lancet. 336:
722-725.
67.Cooke, E.M. 1990. Epidemiology of foodborne illness: U.K. Lancet. 336:790-793. 68.Varabioff, Y. 1990. Incidence and recovery of listeria from chicken with pre enrichment techniques. Journal of Food Protection. 53(7):555-557.
- Gaya, P., Saralegui, C., Medina, M., Nuez, M. 1996. Occurrence of Listeria monocytogenes and other Listeria spp. In raw Caprine milk. J.Dairy Sci. 79:1936-1941.
- Smith, H.R., Rowe, B., Gross, R.J., Fry, N.H., Scotland, S.M. 1987. Haemorrhagic colitis and vero-cytoloxin-producing Escherichia coli in England and Wales. Lancet 1. 1062-65.
- Ärzte Zeitung 1997. Gegen EHEC-Infektionen gibt es noch immer keine spezifische Therapie. Ärzte Zeitung 13. Januar. 1997.
- Coghlan, A. 1996. Animal antibiotics ‘threaten hospital epidemics’. New Scientist. 27 July 1996.
- Ryder, R.W., Blake, P.A., Murlin A.C., et al. 1980. Increase in antibiotic resistance among isolates of Salmonella in the United States, 1967-75. J. Infec. Dis 142:485-91.
- Holmberg, S.D., Osterholm, M.T., Senger, K.A., Cohen, M.L. 1984. Drug-resistant Salmonella from animals fed antimicrobials. New Eng. J. Med. 311(10):617-622.
- Holmberg, S.D., Wells, J.G., Cohen, M.L. 1984. Animal-to-Man Transmission of Antimicrobial-Resistant Salmonella: Investigations of U.S. Outbreaks, 1971-1983. Science 225 No 4644:833-835.
- Ärzte Zeitung 1997. Zahl resistenter Salmonellen nimmt dramatisch zu. Ärzte Zeitung 14. Januar. 1997.
- Vazquez-Moreno, L., Bermudez, A., Langure, A., Higuera-Ciapara, I., Diaz De Aguayo, M., Flores, E. 1990. Antibiotic Residues and Drug Resistant bacteria in Beef and Chicken Tissues. J Food Science 55(3):632-344, 657.
- Manie, T. Khan, S., Brösel, V.S., Veith, W.J., Gouws, P.A. Antimicrobial resistance of microorganisms isolated from retail and abattoir chicken in South Africa. (In Prep). 79.Salisbury, C.D.C., Chan, W., Patterson, J.R, Mac Neil, J.D., Kranendonk, C.A. 1990. Case report: an investigation of chlortetracycline and oxytetracycline residues in suspect swine-slaughtered in Manitoba, Canada, October 1987 to March 1988. Food additives and contaminants. 7(3):369-373.
- Eriksen, J.O. 1990. Antibiotic contamination via the veterinary surgeon as a possible cause of detection of residues in carcasses. Dansk Veterinaertidsskrifts 73(17):911-916.
- Kluge-Berge, S. 1989. Monitoring for contaminants in carcasses as contaminated with heavy metals, organochlorine compounds, organophosphorous compounds, antimicrobial agents, growth stimulants. Norsk. Veterinaertidsskrift 101(1):30.
82 RIDA News. Edit. R-Biopharm GmbH. IV/96
- Prusiner, S.B. 1996. Molecular biology and pathogenesis of prion diseases. TIBS 21:482- 487.
- Riek, R., Horneman, S., Wider, G., Billeter, M., Glockshuber, R., Wüthrich, K. 1996. NMR structure of the mouse prion protein domain PrP(121-231). Nature. 382:180-182.
- Anderson, R.M., Donelly, C.A., Ferguson, N.M., Woolhouse, M.E.J., Watt, C.J., Udy,
H.J., MaWhinney, S., Dunstan, S.P., Southwood, T.R.E., Wilesmith, J.W., Ryan, J.B.M., Hoinville, L.J., Hillerton, J.E., austin, A.R., Wells, G.A.H. 1996. Transmission dynamics and epidemiology of BSE in British cattle. Nature 382:779-788.
- Editorial. 1990. Prion disease spongiform encephalopathies unveiled. Lancet. 336:21-22.
- Will, R.G. and Mathews, W.B. 1984. A retrospective study of Creutzfeldt-Jacob disease in England and Wales 1970-79. I: Clinical features. J.Neurol.Neurosurg.Psychiatry. 47:134-40.
- Masood, E. 1996.’Mad cow’ scare threatens political link between food and agriculture.
Nature. 380:273-274.
- Nature 1996. Lessons from BSE for public confidence. Nature. 380:271.
- Butler, D. 1996. Slow release of data adds to BSE confusion. Nature. 380:370.
- Klaffke, O. 1996. Swiss cull to meet fears of BSE. Nature. 383:289.
- Smith, P.G., Cousens, S.N. 1996. Is The new variant of Creutzfeldt-Jakob Disease from mad cows? Science 273:748.
- Lasmézas, C.I., Deslys, J.P., Demalmay, R., Adjou, K.T., Lamoury, F. Dormont, D., Robain, O., Ironside, J., Hauw,J.J. 1996 BSE transmission to macaques. Nature. 381:743- 744.
- Aguzzi, A. 1996. Between cows and monkeys. Nature. 381:734-735.
- Skegg, D.C.G. 1996. Sacred cows, science and uncertainties. Nature. 382:755-756.
- Masood, E. 1996 BSE transmission data pose dilemma for UK scientists. Nature 382:483.
- Wise, J.1996. Scientists find low level transmission of BSE. BMJ 313:317.
- Kluger, J. 1997 Could mad-cow disease spread further? Time. January 27, 1997.
- Butler, D. 1996. Statistics suggest BSE now ‘Europe-wide’. Nature. 382:4
- Stekel, D.J., Nowak, M.A., Southwood, T.R.E. 1996. Prediction of future BSE spread.
Nature. 381:119.
- Skovgaard, N. 1989. Future prospects for meat inspection. Possibilities and trends.
Dansk Veterinaertidsskrift 72(5):241-249.
- Pursel, V.G., Pinkert, C.A., Miller, K.F. et al 1989. Genetic engineering of livestock.
Science. 244:1281-87.