Milk and dairy products are advertised as wonder foods that will supply all the nutrients required for healthy growth. The calcium levels in milk, in particular, are stressed as an essential component of the human diet, and the impression is created that a loss of this dietary source of calcium will lead to abnormal bone development. It is certainly true that dairy products are packed with nutrients, but this does not mean that the combination of nutrients is suited to human nutrition. Mother’s milk is essential for infants, but then infants are specially designed to cope with this growth-promoting food. Prior to weaning the necessary enzyme systems needed for the digestion and assimilation of milk components are active, but they are progressively deactivated with age. The milk of other mammalian species also differs in composition from mothers milk, and this, together with the potential danger from ingested antigens, makes cows milk unsuitable for human consumption.
There is considerable resistance from industry, and even from the established scientific world, to the idea that dairy consumption is detrimental to health, but the evidence from recent scientific findings seems fairly conclusive with regard to this issue. Dairy consumption is being coupled with a host of diseases, and as consumption rises world-wide, so the evidence is becoming more and more conclusive. In the past, the detrimental effect of the consumption of dairy products may have been masked by the positive effects of other lifestyle choices such as higher consumption of grains, fresh fruits and vegetables with their high fibre content. Western diets have, however experienced a sharp increase in the consumption of animal products, including dairy products, with concomitant decline in the consumption of grains, legumes, fruits and vegetables, and this may explain the increase in the incidence of degenerative diseases in industrialized countries.
Lactose intolerance
Lactose, the sugar in milk, is broken down in the intestines by the enzyme lactase. Most people are able to digest lactose properly during infancy and early childhood, but as they grow older this ability declines. Approximately 75% of adults worldwide are lactose intolerant and those with the highest intolerance are Native Americans and Asians and only slightly lower than these are the blacks, Jews, Hispanics, and southern Europeans. Lactose intolerance is lowest among northern Europeans and their descendants. In the US some 25% of Caucasians, 51% of Hispanics and 75% of all African Americans, Jews, and Native Americans have insufficient levels of lactase to digest dairy products and 90% of Asian Americans are lactose intolerant.20,21 It has been found that 90% of African people are lactase deficient, and in the case of the rural Zulu of South Africa it was found that they showed no change in blood glucose concentrations after ingesting 50g of lactose.22 When milk and dairy products are digested, lactose is broken down by the enzyme lactase into glucose and galactose (fig. 4.8).
The presence of lactose is a feature of mammalian milk, but the concentration of this sugar is normally geared to the needs of the species, as are the concentrations of all the other components of milk. In the case of humans, mother’s milk does not only contain the essential nutrients that are required for growth and development, but also contains the bacterium bacillus bifidus that assists in the digestion of lactose. In cow’s milk, however, the bacterial composition differs from that of human milk, and if cow’s milk is fed to infants, this can interfere with the digestion of lactose. Moreover, human milk has a higher carbohydrate concentration (7%-7,5%) than cow’s milk (4,5%-5%) and contains some 200m mol/litre of lactose which makes it sweeter than cow’s milk. The lower protein and higher carbohydrate content of human milk is also more suited to the needs of infants, because their growth rates are considerably lower than those of calves.
After the conversion of lactose to glucose and galactose, the available galactose is not utilized as such, but is converted to glucose in the liver by a series of steps requiring the initial presence of the enzyme galactokinase. The production of both the enzymes lactase and galactokinase declines with age, and the capacity to digest and utilize the products of lactose in adult life is thus curtailed. A deficiency in the enzyme lactase will result in fermentation of lactose by intestinal bacteria, which can result in abdominal distress such as the development of excessive gas, cramping, bloating, borborygmi (stomach rumbling), altered bowel habits and diarrhoea.21 The severity of the symptoms depends on the quantity of lactose consumed and the level of intolerance.
Milk protein intolerance
A further problem with milk is encountered in the digestion of the milk protein casein. In comparison to human milk, cow’s milk contains 300% more casein and more than double the amount of total protein. Casein and β-lactoglobulin are the two main proteins in milk and they are unique in that they contain a perfect blend of amino acids, which is precisely what is needed during early infant growth. Human infants, however, double their mass on average 180 days after birth, whereas cows achieve the same feat in only 47 days. Cow’s milk is therefore geared to meet the rapid growth requirements of cows, but is not suitable for humans. Casein also naturally stimulates normal thyroid function in infants, and as the thyroid is involved in many developmental processes, including the development of the nervous system, casein from other mammalian species could have adverse effects on metabolic processes of infants particularly since a portion of the dietary casein can be absorbed undigested and serve as antigen.
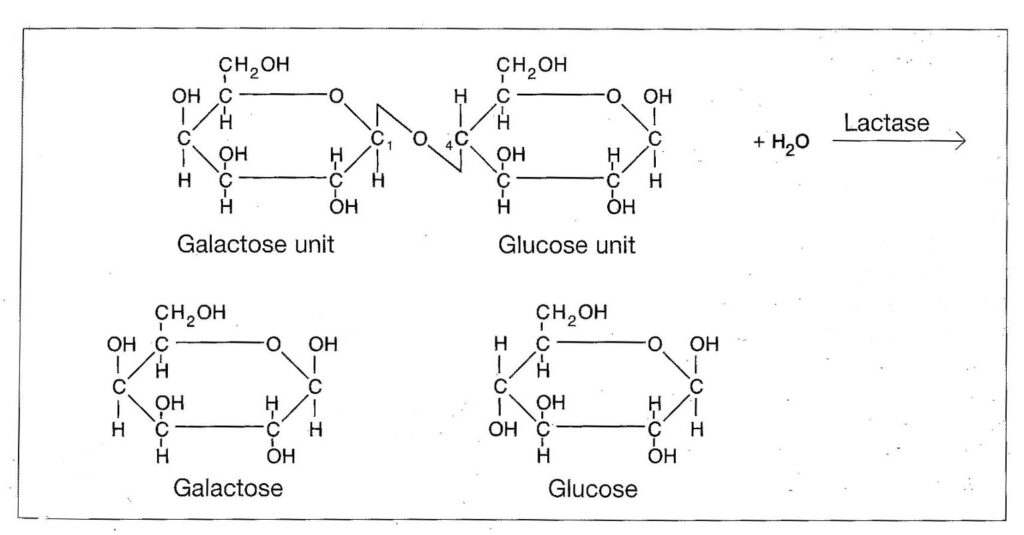
Figure 4.8. The digestion of lactose.
As is the case with the enzyme lactase that digests lactose, the concentration of the enzyme rennin, that breaks down the casein, also declines with age in all mammals, and by the time milk teeth develop it is virtually non-existent in the human digestive tract. Without rennin, the digestion of casein has to be carried out by the normal proteolytic enzymes which are not as efficient in breaking down casein. The presence of casein in the diet of mammals has also been linked to elevated cholesterol levels and various degenerative diseases such as arteriosclerosis. Rabbits fed casein developed arteriosclerosis, but the effect could be reduced if a plant protein source, such as soybean flour was introduced into the diet. This shows, that the amino acid pool produced by casein probably no longer meets the requirements of weaned or adult mammals. Casein also produced higher cholesterol levels than soy protein in a number of animal species, including rats, hamsters, guinea pigs, pigs, and monkeys. In humans, a reduction in cholesterol levels was also found if meat and dairy proteins were replaced by soy proteins.23,24 Casein also seems to have an adverse effect on insulin secretion, thyroxine levels, gastrointestinal hormones and it has an adverse effect on calcium metabolism.
Calcium in dairy products
A matter which has received much media attention, is the calcium content of milk and dairy products. It certainly is true that dairy products do contain fair amounts of calcium, but a large proportion of the calcium in milk is combined with casein in the form of calcium caseinate. Dairy products are also not the only source of calcium available to humans, as grains, legumes, seeds, nuts and many vegetables are excellent sources of calcium. Moreover, fractional absorption of calcium from these sources is higher than from milk. A study done on whole-wheat products showed that fractional calcium absorption from whole-wheat bread exceeded the absorption of calcium from milk, ingested at a comparable load, in the same subjects.25 Not only is the absorption rate of calcium higher from plant sources, but animal sources seem to cause calcium loss in view of the nature and the concentration of the proteins which they contain. Table 4.3 lists the calcium levels in some dairy products and plant foods.
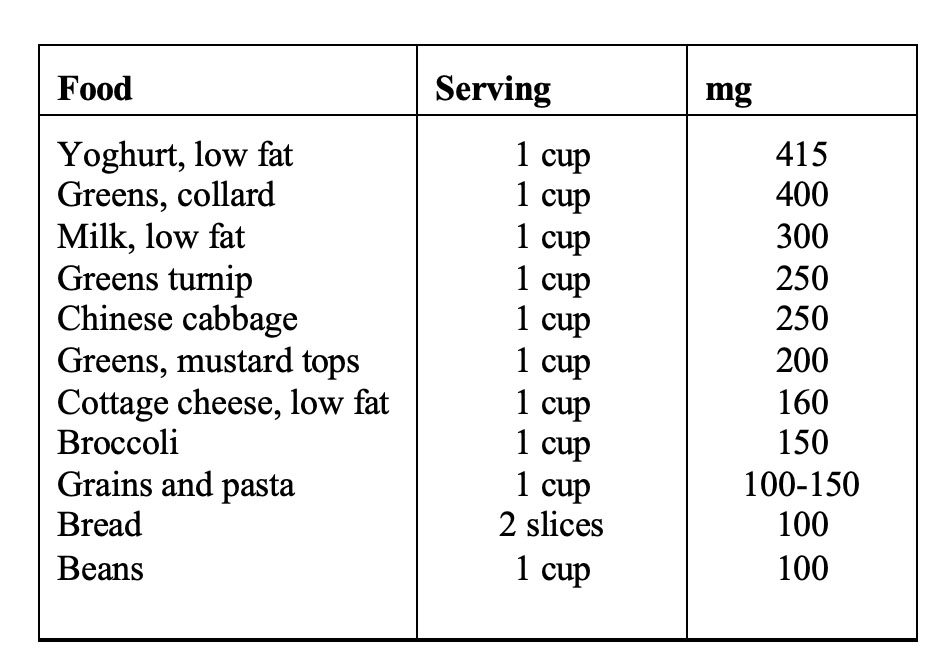
Table 4.3. Calcium levels in selected foods. (From reference 26)
Foods vary in their composition, and in the case of seeds, grains, beans and vegetables, there are considerable differences in calcium content of different varieties and in general, dark green vegetables are a good source of calcium. In addition to the foods listed above, almonds, sesame seeds, sunflower seeds, soybean products such as bean curd and soy flower, carob, chick peas, haricot beans, mung beans, garlic, parsley, watercress and dried fruits (especially figs) are good sources of calcium.
Calcium utilization is governed by complex processes, and the absorption, bone deposition and excretion of calcium is strongly influenced by other dietary components. It is well documented that increased protein consumption causes calcium loss in the urine,27,28 and this is particularly true in the case of proteins from animal products.29 An investigation into the effects of various protein diets on calcium retention showed that proteins from dairy products, such as cottage cheese, caused considerable calcium loss in the urine.30 The culprit here seems to be casein, and other studies seem to corroborate this. In one study it was found that casein fed to weanling rats caused kidney calcification, an effect which was not observed if the protein came from another source.31 If calcium losses exceed absorption, then a negative calcium balance exists, and calcium must be mobilized from bone in order to maintain plasma calcium levels in a dynamic state. This loss of calcium from bone can eventually lead to osteoporosis. It is, therefore, not surprising that osteoporosis seems more prevalent in countries where the consumption of dairy products is high.32,26 In table 4.4 the incidence of osteoporosis in various countries in relation to the consumption of proteins and dairy products is presented, and in figure 4.9, the relationship between dairy consumption and osteoporosis (expressed as hip fracture rate per 100 000 women) is presented.
Although dairy products are rich in calcium, paradoxically, it is apparent from the above data that the calcium from milk is not synonymous with healthy bone structure (see chapter 5 for more information on dairy free diets and osteoporosis). Moreover, calcium supplementation does not provide a solution for the dilemma, as countries, such as the United States, with the highest supplementation rates still have among the highest rates of osteoporosis. Not even in lactating women does calcium supplementation seem to have much of an effect in either white or black women. In one study on White, middle class women it was found that absorption of calcium from the intestines was not increased during supplementation compared to lactating women on low calcium diets. The calcium needs for milk production were met by decreased urinary excretion and increased bone resorption and not by increased intestinal absorption despite high calcium intakes.33
In a study on Gambian women similar results were obtained. Gambian women normally have a low calcium diet based largely on rice, millet, groundnuts and fish. This diet provides less than 300 mg/day of calcium which is considerably lower than current recommendations for lactating women. Increasing the calcium level threefold to bring it line with FAO/WHO recommendations had no discernable effect on breast milk calcium concentrations or on the maternal bone mineral content. This suggests that there was no benefit from increasing the calcium intake during lactation.34 The women in the supplementation group had consumed a total of 0.26 kg (one quarter to one third of the whole- body calcium content) after 52 weeks, and showed significantly greater urinary calcium output (7% of the dose). As the bone mineral content did not change, the researchers concluded that the rest of the additional calcium was just not absorbed from the intestinal tract.34 This study underlines the fact that calcium needs can be adequately met by even low calcium diets that contain no dairy products.
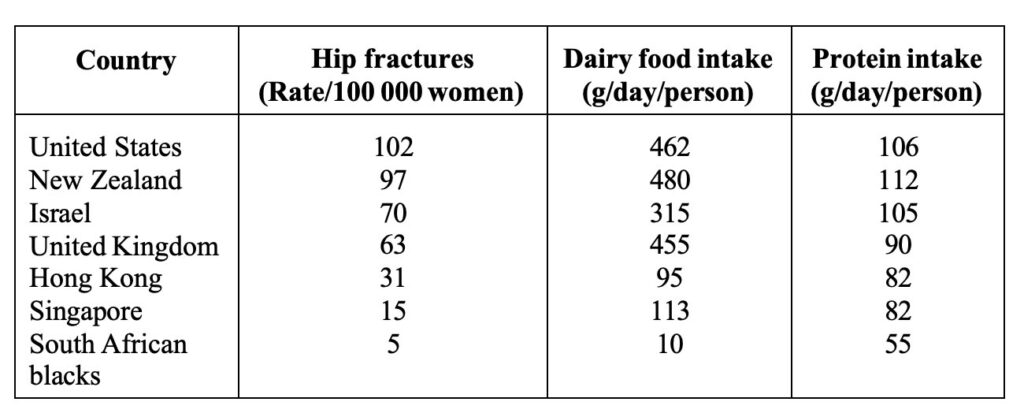
Table 4.4. Correlation between osteoporosis, dairy food and protein consumption by countries. (Adapted from reference 26).
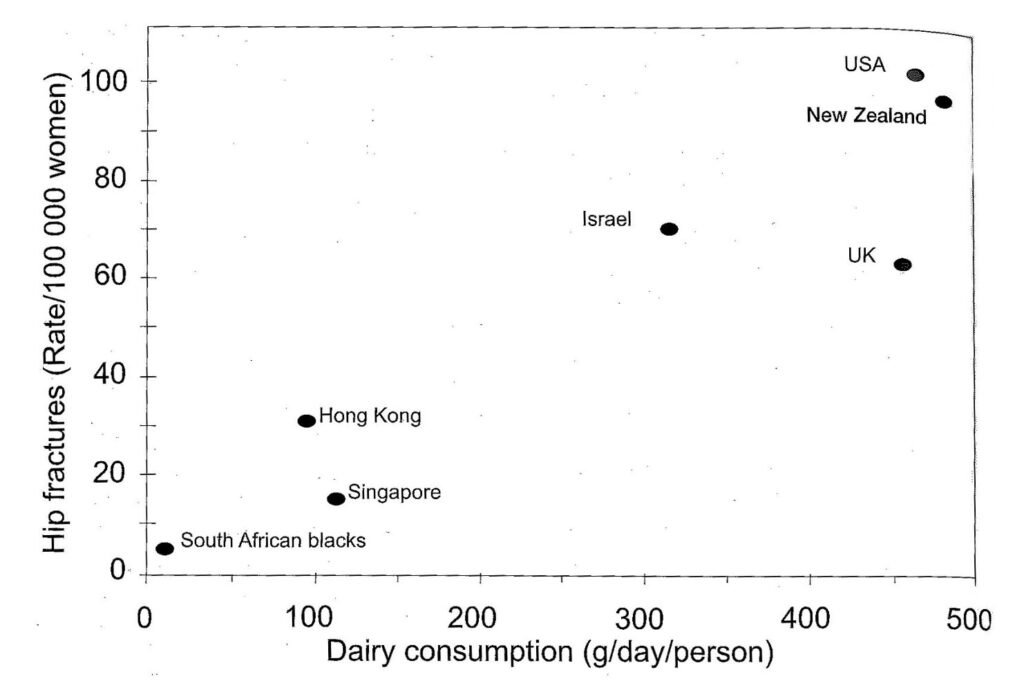
Figure 4.9 Correlation between osteoporosis and dairy food consumption by countries. (Adapted from reference 26).
In our own laboratory we have consistently found that animals (sheep, rats, rabbits and vervet monkeys) fed animal proteins, particularly casein or dairy products showed significant increases in urinary calcium levels, compromised bone status, and in common with the other studies, reduced intestinal absorption. In a current study on Vervet monkeys conducted at the Primate Unit of the Medical Research Council in South Africa two groups of monkeys were fed diets containing equivalent quantities of calcium, but one group received largely milk powder as protein source whilst the other group received kidney beans and maize as protein source. Stool calcium analyses showed that absorption of calcium was significantly lower in the dairy group than in the bean/maize group irrespective of whether they were on a high (17%) or low (8%) protein diet thus demonstrating the adverse effect of dairy products on calcium utilization.35
Dairy products and the immune system
Human milk not only contains less protein than cow’s milk, but the distribution of proteins is also different. A group of proteins that are particularly important in this regard are the immune globulins which carry antibodies and are particularly numerous in the early milk known as colostrum. These globulins contain antibodies found in the mother’s blood and transmit immunity to the newborn infant. When mother’s milk or cow’s milk is ingested, the system is capable of transporting these antibodies directly into the blood-stream via carrier systems, an ability that persists to a lesser extent even in adults. Human milk contains antibodies which differ from those found in cow’s milk and when cow’s milk is substituted for mother’s milk, the immunoglobulins from the cow’s milk will interact with the immune system and this can lead to an allergic reaction. Many allergies can primarily be attributed to milk, and will disappear when milk is removed from the diet.
Allergic disorders are a widespread health problem of particularly infants and young children in the developed world, and according to several population studies, the incidence and severity of these disorders has increased significantly of late.36 Cow’s milk is a major source of allergies and has been implicated in virtually all the common ailments of the respiratory tract. Hay fever, sinusitis, chronic bronchitis, colds, ear infections and even asthma can largely be ascribed to the intake of dairy products.37,38,39 In addition to these ailments, children are prone to diarrhoea, vomiting, constipation, colic, growth retardation, psychological disturbances, eczema and asthma if fed cow’s milk. Allergies need not immediately be apparent and can manifest later in life. Moreover, once an allergic reaction to a substance is manifested, greater sensitivity to other antigens is induced.37 A causative factor in congestive diseases is the ability of dairy products to promote mucus formation, and milk, cheese, butter and cream are the most likely of all foods to promote the build up of mucus.
Cow’s milk also causes colic in infants. The relationship between cow’s milk and colic is well established, and in infants that are breast fed, but also receive cow’s milk, colic is very common. Once cow’s milk is removed from the diet, however, colic disappears in most cases.40 Cow’s milk allergy is frequently the first manifestation of allergy because the proteins in cow’s milk are the first foreign antigens encountered in large quantities in infancy.36 Allergy to cow’s milk is most prevalent at the age of 1 year and has been reported in 2.8% of the general child population, but in infants with atopic dermatitis the incidence of cow’s milk allergy is at least five times that figure.36 Atopic dermatitis is a chronic eczematous skin disease which frequently begins in infancy and probably results from the repeated ingestion of allergins. This in turn leads to frequent scratching and the consequent
trauma induced lichenified lesions. It has been established that casein from cow’s milk causes an increase T-cell frequency and a specific T-cell-mediate immune response to casein can be found in the blood of adolescent and adult patients who suffer from milk-related exacerbation of atopic dermatitis.40
Cow’s milk has been linked to the development of insulin-dependent diabetes (IDD). IDD results from a chronic autoimmune process that can exist for years in a preclinical phase, with the classic manifestations of the disease (hyperglycaemia and ketosis) only occurring after most of the insulin-producing beta cells have been destroyed. There is evidence, that T lymphocytes are a major contributor to the pathogenic process. In this regard, cow’s milk has received much attention because people who were not breastfed or breastfed for only a short period of time are at increased risk of IDD. It is noteworthy, that 100% of newly diagnosed patients with IDD have antibodies to bovine serum albumin. Moreover, the pancreatic beta- cell proteins display substantial molecular cross-reactivity with bovine serum albumin from cow’s milk. IDD can thus be an abnormal response to the foreign protein leading to an immune response to both bovine serum albumin and the pancreatic beta-cell protein. 41
The findings by Cavallo et al 42 of peripheral blood T-cell reactivity to β-casein in half their 47 patients with IDD adds weight to the cow’s milk hypothesis.43 There have been arguments for and against the cow’s milk hypothesis, since IDD also occurs in infants that have never received cow’s milk. However, it has now been conclusively shown that the antigens in cow’s milk are transferred to the mothers milk if she consumes cow’s milk. In a study done on Japanese women it was found that β-Lactoglobulin was transferred to the mother’s milk because it is resistant to acid and enzymatic degradation and if taken orally is absorbed into the system.44 Moreover, there have been reports of infants that are only breastfed and never received milk protein developing allergies to cow’s milk, which was then alleviated when the mothers eliminated dairy products from their diets.44
Finally, the consumption of dairy products has been implicated in intestinal ulcers45 and cancer. Milk consumption in particular has been positively correlated with prostate cancer,5 and in an Italian case study, risk of breast cancer was positively associated with the intake of milk and dairy products.46 For infants, the best food is mothers milk and cow’s milk should be avoided at all costs. Mothers milk will ensure the normal development of infants at every level. It has even been established that the intelligence quotients (IQ) of children that were fed breastmilk are significantly higher than those of children that did not receive breastmilk even after adjustment for differences between groups, mother’s education and social class. 47 For those that have become accustomed to the consumption of milk, the replacement of dairy products with legume, seed or nut milks and creams will provide a more than adequate alternative to milk.
Dairy products and infertility
The issue of a rise in infertility, particularly male infertility, has produced considerable controversy in scientific circles. More and more reviews have appeared in the scientific literature claiming a decline in semen quality which is being largely attributed to environmental factors such as exposure to oestrogens (dietary, pharmaceutical and environmental pollutants). It has been suggested that environmental factors, possibly acting in fetal and early neonatal life, may be responsible for the negative effects. Some researchers have claimed that the statistical methodology employed to determine the decline in semen quality was incorrect and that no real decline had taken place over the last decades. To investigate this claim, a group of researchers from the University Department of Growth and Reproduction and the Statistical Research Unit in Copenhagen Denmark, systematically
reviewed the complete international literature on semen analysis since the 1930’s using rigorous selection criteria and statistical analyses. They found, that linear regression of data weighted by the number of men in each study showed a significant decrease in mean sperm count from 113 X106/ml in 1940 to 66 X 106/ml in 1990 (p≤ 0.0001) and in seminal volume from 3.40 ml to 2.75 ml (p=0.027), indicating an even more pronounced decrease in sperm production than expressed by the decline in sperm density. They concluded, that there had been a genuine decline in semen quality over the last 50 years.48
The Danish study was subsequently also criticised with regard to the statistical methodology employed,49 but the issue would still not come to rest. A group of researchers from the MRC Centre for Reproductive Biology in Edinburgh, on the strength of the arguments against the statistical methodologies employed, regrouped the data to account for the year of the donor’s birth and found a similar decline in sperm concentration as reported by the Danish researchers,50 and all the trends seem to point to a decline in the health of the male reproductive system.51 It is true that a number of investigations, particularly with regard to the United States, have not shown a decline in semen quality,52,53,54 but overall the evidence is overwhelming that reproductive health is on the decline. An analysis of semen quality among fertile men in Paris using sperm stored in the sperm bank, showed that between 1973 and 1992 there had been no decline in semen volume, but that sperm concentration, motility and the percentage of morphologically normal spermatozoa had declined significantly.55
Of interest is also an observation that some nations experienced a greater decline than others in terms of semen quality a notable example being the comparison between Finland and Britain, where it has been reported that the British men are less fertile than those from Finland.56 Even in Finland, it has however been reported by researchers from the Forensic Department of the University of Helsinki, that the findings from post mortem analyses of two groups of men from 1981 and 1991 showed a dramatic decline in overall reproductive health. The researches reported that not only the number of men with normal spermiogenesis had declined by more than half, but the frequency of pathological disorders of the testes had increased.57 The precise reason for the overall decline, as well as differences between nations in reproductive health have not been clearly established. The main argument revolves around environmental oestrogens,58 but although this may be a contributing factor, even this hypothesis is still being considered as guesswork at this stage.59 The strongest evidence for the oestrogen argument is that the sons of women who were given high doses of diethylstilboestrol in the first trimester of pregnancy to prevent spontaneous abortions, have a high incidence of reproductive abnormalities.60 The main factors for male infertility are summarised in table 4.5.
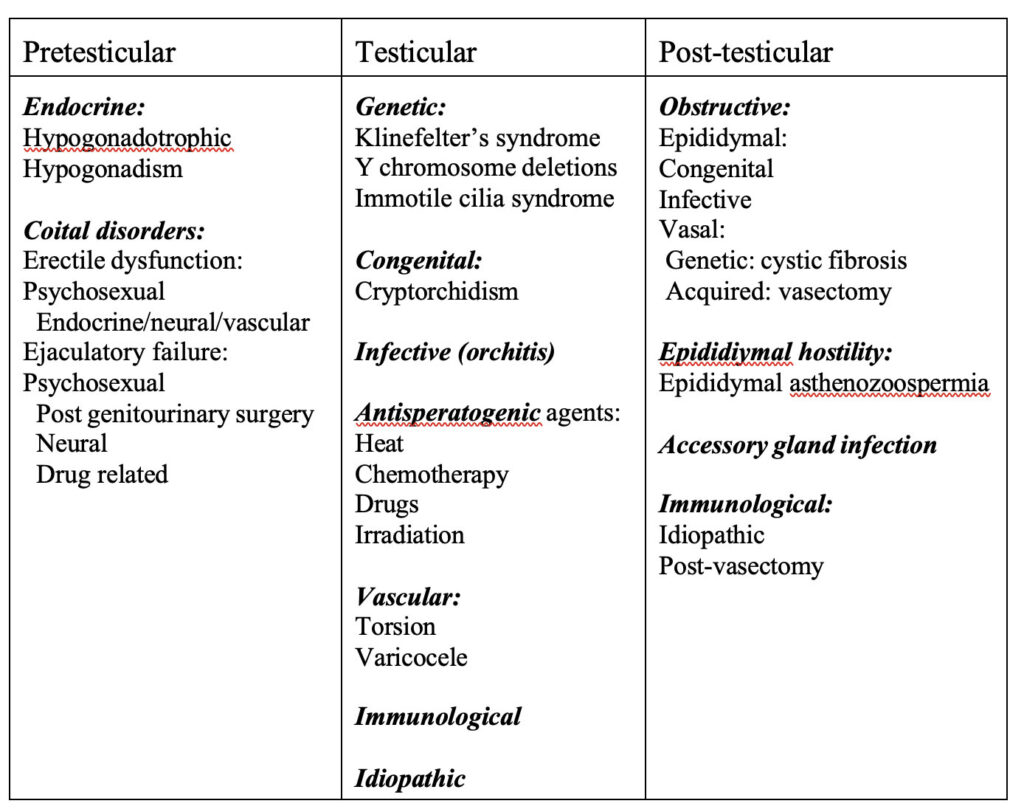
Table 4.5. Aetiological factors in male infertility. (From reference 61)
Although male infertility has received so much attention of late, female infertility is even higher than that of males. One couple in 10 seeks medical help because of infertility and a 1982-85 multicentre study by the World Health Organization found that in 20% of cases the problem was predominantly male, in 38% the problem was predominantly female, in 27% abnormalities were found in both partners and in the remaining 15% no clear-cut cause of infertility was identified.62 Although environmental pollutants and oestrogenic drugs may play a significant role in the decline in fertility, other factors, such as changes in diet, may be equally significant.
There have been significant changes in the consumption of animal products in Western societies over the last decades, and the consumption of dairy products in particular has increased dramatically. Fat consumption has also seen a significant increase in the past decades (see chapters 3 and 5) and these dietary changes have been associated with increased risk of degenerative diseases. Male prostate pathology has been linked to the consumption of dairy products,5 and this led us to investigate the possible link between the consumption of dairy products and reproductive health. The study was conducted on vervet monkey at the Primate Unit of the MRC in South Africa, so as to get as a close a model to the human as possible. Twelve monkeys were divided into two groups of six individuals each and they were put on diets containing 17% protein. The one group received largely maize and legumes and the other group milk powder as protein source. In order to assess the impact of high and low protein concentrations, after an initial two month period the protein allocation was
dropped to 8% from the respective sources and analyses were continued for an additional two month period. In this way the long- and short-term impact of the consumption of dairy products on reproductive health could be assessed. Already in the short-term, a significant decline in sperm quality, motility and concentration could be discerned, and these preliminary results were reported at the 6th International Congress on Cell Biology and 36th American Society for Cell Biology Annual Meeting held in San Francisco USA in 1996.63
When protein concentrations were high, the sperm concentrations between the two groups of monkeys were not significantly different, but progressive motility and the number of defective spermatozoa (particularly midpiece defects) increased. When protein concentrations were lowered to 8% crude protein, the group on dairy experienced a significant decline in sperm concentration, whilst the group on legume and maize showed no drop in sperm concentration and even showed an improved motility. Moreover, the number of defective spermatozoa also increased in the dairy group. In figures 4.10 and 4.11 the sperm progressive motility and the sperm concentration of the two groups of vervet monkeys is shown for the first four month period.
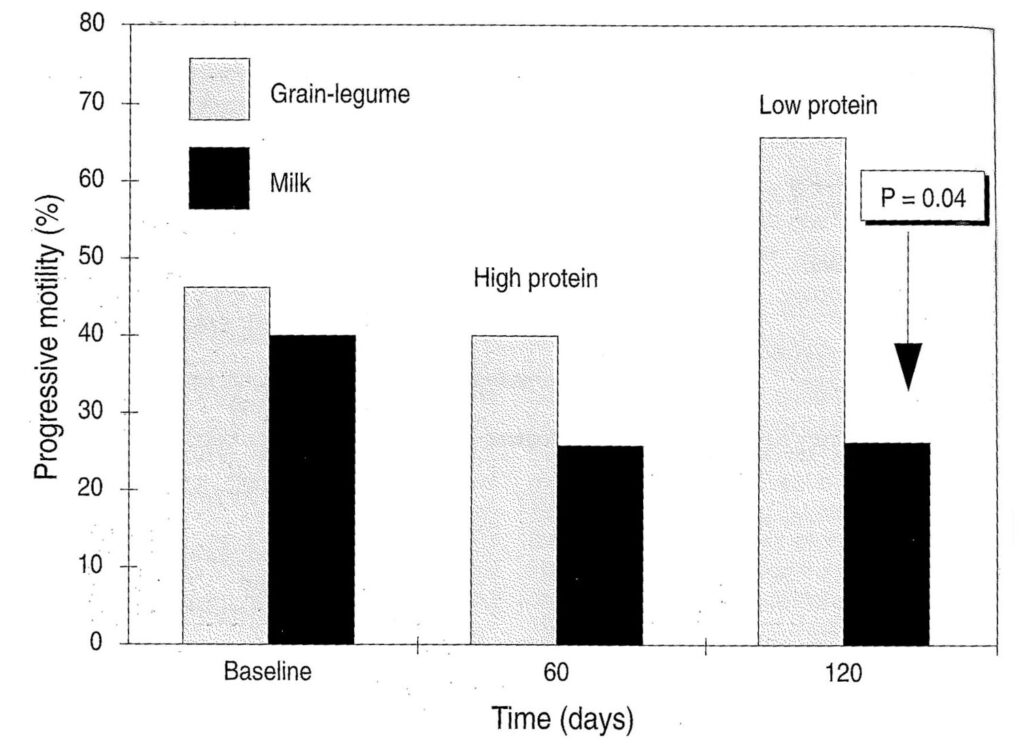
Figure 4.10. Progressively motile sperm of monkeys on milk and legume plus maize diets as protein source. (P=0.04 verified via the Wilcoxin 2-sample Test) The baseline represents the status of the animals at the start of the experiment before the introduction of the new dietary regime. (From reference 35).
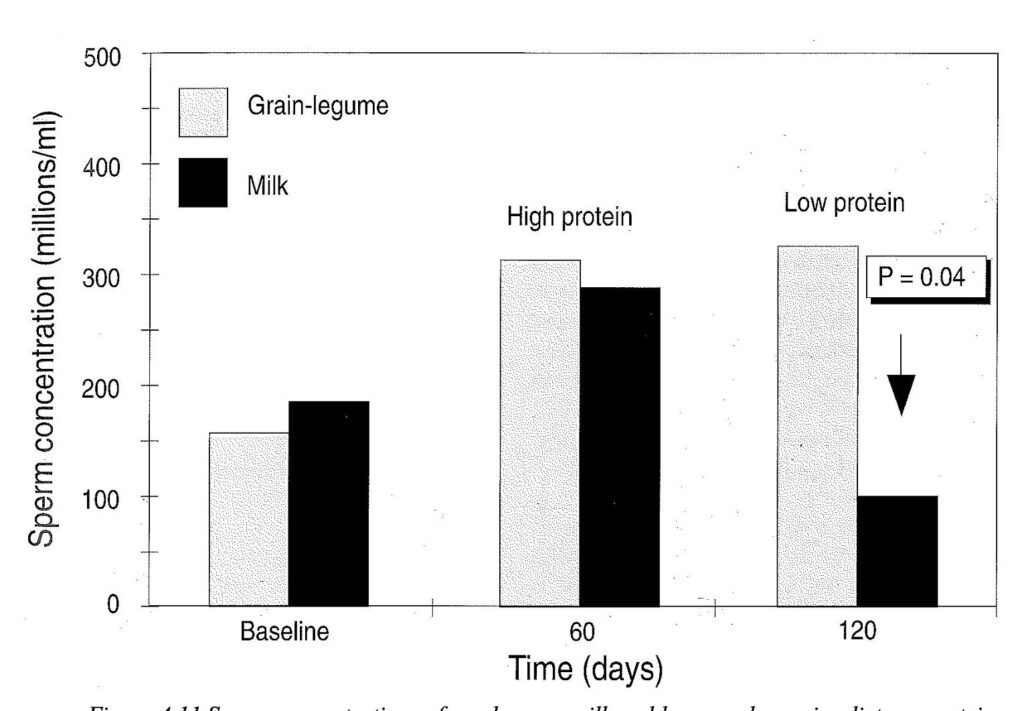
Figure 4.11 Sperm concentrations of monkeys on milk and legume plus maize diets as protein source. (P=0.04 verified via the Wilcoxin 2-sample Test) The baseline represents the status of the animals at the start of the experiment before the introduction of the new dietary regime. (From reference 35).